
Fibrous dysplasia is a fibro-osseous medullary lesion; it affects a single bone (monostotic) in 70% of cases and more than one bone (polyostotic) in 30% of cases. Polyostotic fibrous dysplasia manifests in association with skin hyperpigmentation and endocrine abnormalities in McCune-Albright syndrome. Fibrous dysplasia in the craniofacial bones accounts for 35% of monostotic fibrous dysplasias, even if it involves several adjacent bones. The skull base and facial bones are common sites of involvement, and in this setting, they may encroach on the nasal cavity. The jaws are the most frequently affected bones. Fibrous dysplasia is more common in the 1st and 2nd decades of life and has a slight female predilection.
The clinical manifestations of fibrous dysplasia include painless swelling, facial deformity, exophthalmos, and symptoms related to narrowing of skull base foramina. Fibrous dysplasias that undergo periods of increased activity can cause increased swelling and discomfort and may mimic osteomyelitis on bone scans. The growth of this lesion tends to decrease after puberty. The diagnosis is confirmed by the presence of the mutation of GNAS 1α, which enables the differentiation of fibrous dysplasia from other fibro-osseous lesions.
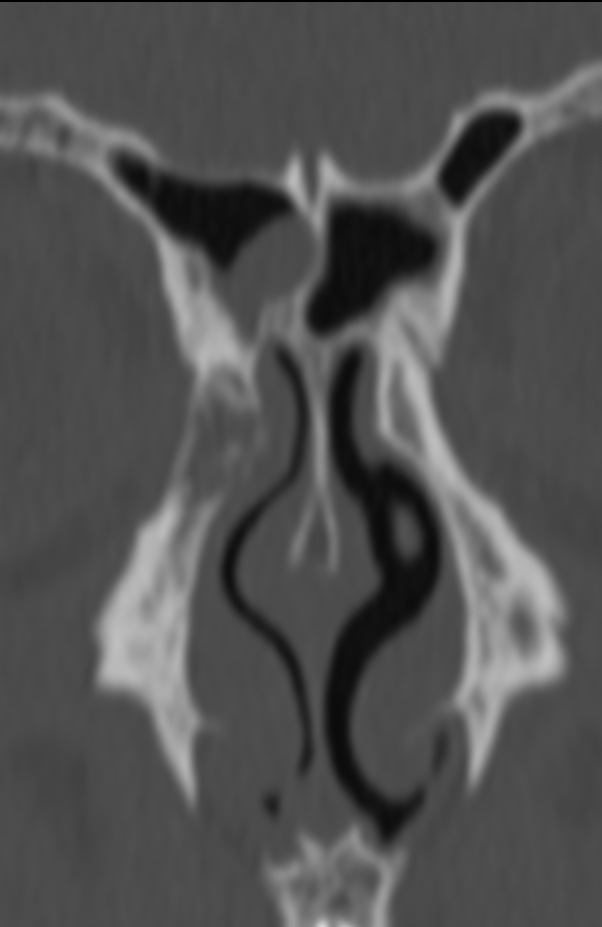
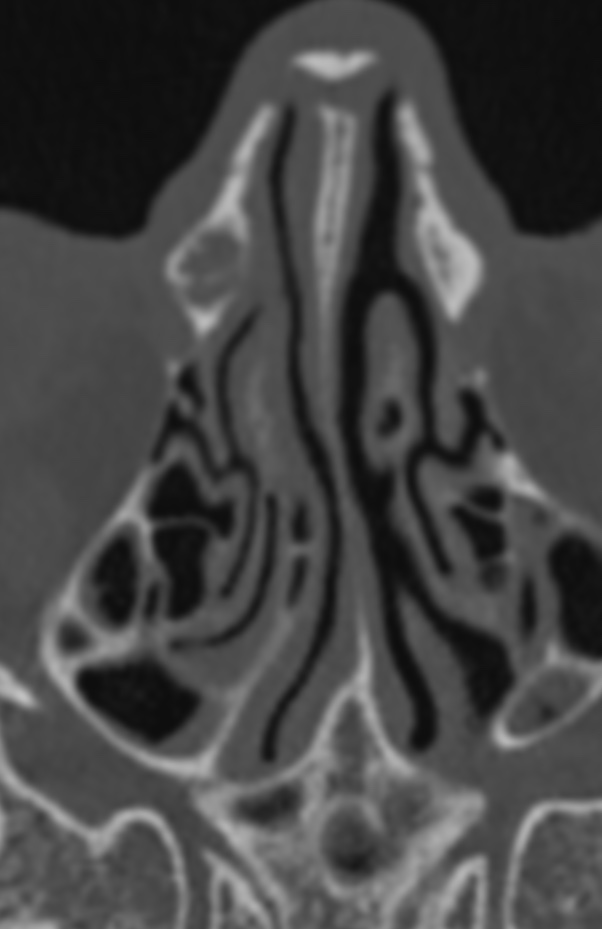
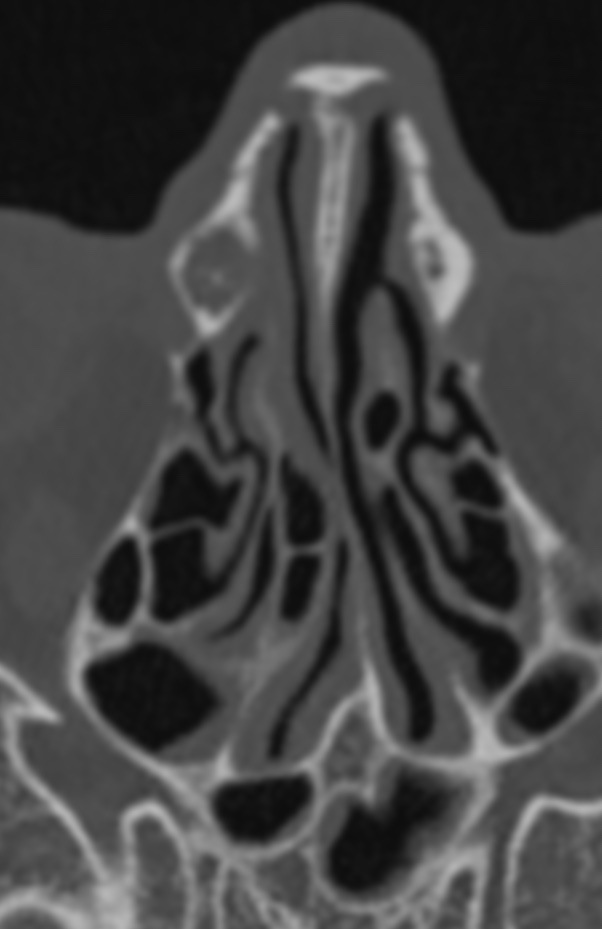
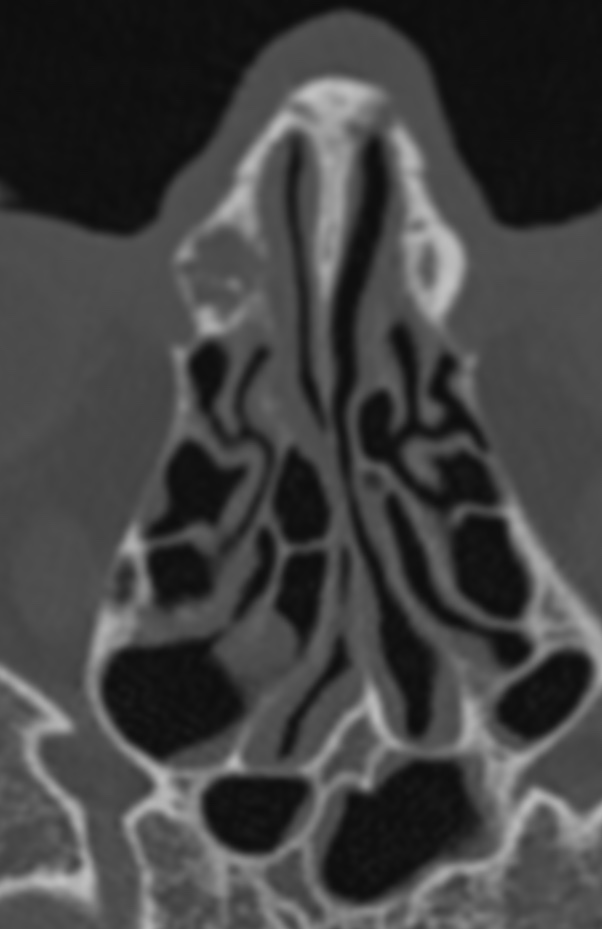
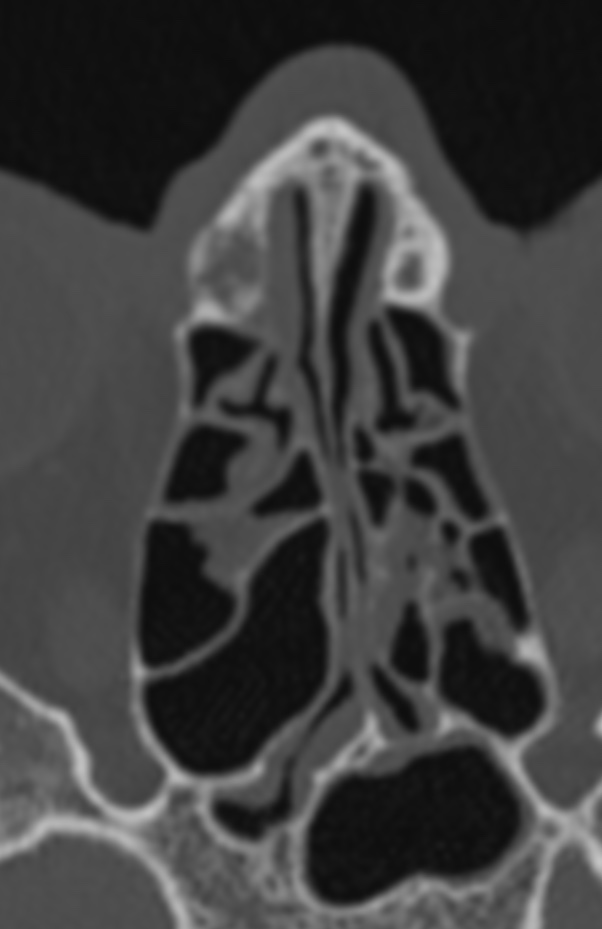
The imaging characteristics of fibrous dysplasias depend on the stage of development of the disease and the amount of bone matrix, and vary from lucent to sclerotic lesions. At plain radiography and CT, this lesion has the characteristic ground-glass appearance, which is secondary to the amount of woven bone present. Fibrous dysplasia manifests as an expansile lesion that has ill-defined margins and a thinned cortex; it replaces normal bone but rarely involves bone erosion. CT is key to rendering an accurate diagnosis, given that fibrous dysplasias can exhibit aggressive characteristics at MR imaging, mimicking malignant lesions.
At MR imaging, the appearance of fibrous dysplasia is variable, but it typically has low signal intensity on T1-weighted images. The signal intensity is variable on T2-weighted MR images: it can be low, intermediate, or high. At contrast-enhanced imaging, there is internal heterogeneous enhancement, with the fibrous component typically enhancing more than the osseous component. As a benign lesion, fibrous dysplasia has increased diffusivity on apparent diffusion coefficient maps, which can help in differentiating it from a malignant lesion.
Reference: