Epidermoid tumors arise from ectoderm trapped within/displaced into the central nervous system. They show predilection for CPA Angle (up to 40%), 4th ventricle, suprasellar region, and spinal cord. They are the 3rd most common CPA tumor, comprising approximately 7% of CPA pathology. CPA lesions can produce 5th and 7–12th cranial nerve neuropathies.
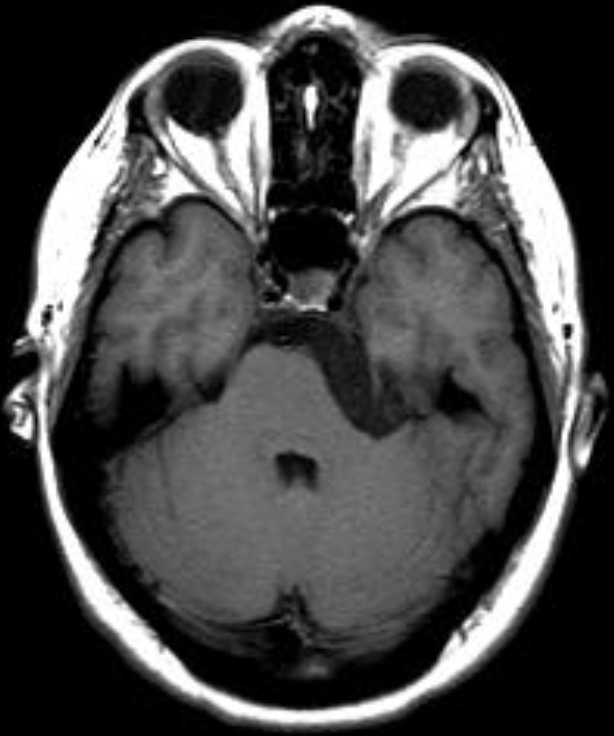
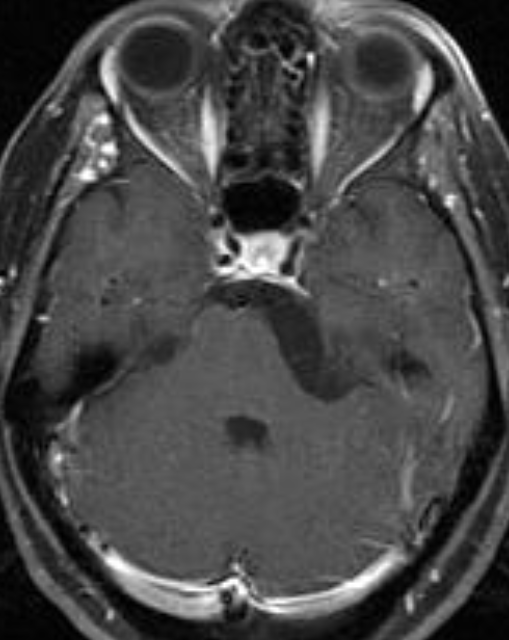
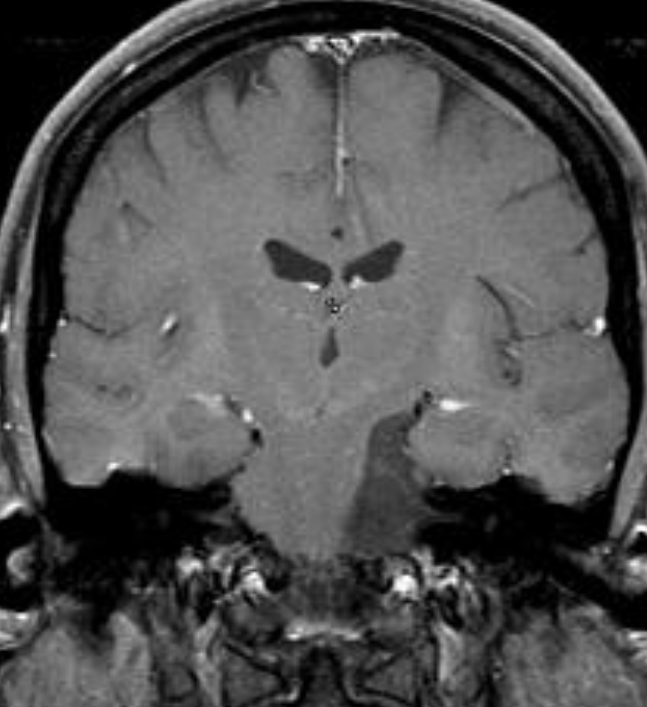
Recurrent episodes of aseptic meningitis caused by cyst content rupture may occur. Symptoms include fever, meningeal irritation, and hydrocephalus. A 26-year-old female presented with headaches. Head magnetic resonance imaging (MRI) revealed right CPA tumor with brain stem compression. There was evidence of restricted diffusion in diffusion-weighted imaging, typical of epidermoid tumor.
The tumor grows slowly and is soft and very pliable, conforming to the shape of the adjacent brain and CSF spaces in which it is growing. The cysts, frequently referred to as “pearly tumors” because of their gross external appearance, account for approximately 0.2% to 1.8% of brain tumors. Although
congenital in nature, they usually do not present clinically until the third or fourth decade. The cysts may be extradural or intradural in location. The intradural lesions are frequently located in the cisterns of the cerebellopontine angle, supra- and parasellar regions, and middle cranial fossa, as well
as the cisterna magna. Tumors may also develop in the tela choroidea, usually in the temporal horn of the lateral ventricle but occasionally in the fourth ventricle.
On CT the lesions are hypodense and do not enhance with contrast material. They are difficult to differentiate from arachnoid cysts based on their density; however, their external surface is usually lobulated in configuration compared with the smooth surface of an arachnoid cyst. There may occasionally be focal calcifications in their walls. In contrast to arachnoid cysts, epidermoids tend to engulf and surround vessels and cranial nerves, whereas arachnoid cysts displace such structures.
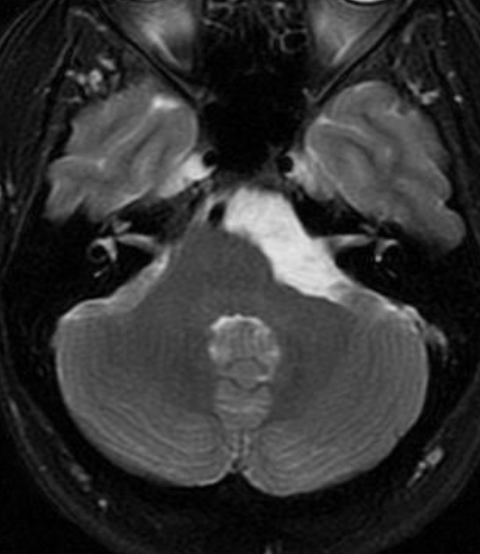
On T1-weighted MR images, epidermoid tumors demonstrate subtle hypointensity compared to CSF. There is usually mild inhomogeneity of low intensity, with some patchy regions of isointensity within the lesion. On T2-weighted sequences the tumors show marked hyperintensity similar to or greater than that of CSF, with significant heterogeneity of the signal.
The low-intensity signals within the tumor hyperintense pattern are probably the result of the cellular
debris and solid cholesterol crystals within the cysts . A high-intensity rim may surround the portion of the cyst on T2-weighted sequences that probably represents a CSF cleft. The tumors may be dumbbell shaped in configuration and extend from the middle cranial fossa into the posterior fossa. They may have a smooth external surface but in most instances demonstrate a lobulated appearance. No free fatty
acids have been found in epidermoid cysts that are of low intensity on the T1-weighted sequences. On MRI, epidermoids are distinctly different from arachnoid cysts, in that epidermoid tumors are virtually never isointense to CSF on MR images when using FLAIR. In addition, diffusion- weighted imaging demonstrates reduced diffusion within epidermoids, simplifying the diagnosis and aiding visualization.
Reference:
Atlas S. Chapter 11: Adult Brain Tumors p581