
Thyroid goiters are estimated to occur in approximately 5% of the population worldwide . Most are in the neck, yet between 3% and 17% of these goiters extend into the thorax and are also called substernal, particularly when more than 50% of the mass is below the suprasternal notch . Intrathoracic goiters are
usually in the anterior mediastinum. A small subset of 10-25% may be found in the posterior mediastinum Radiologic imaging is an important step in the workup of these patients because the surgical approach depends on the location and size of the intrathoracic goiter.
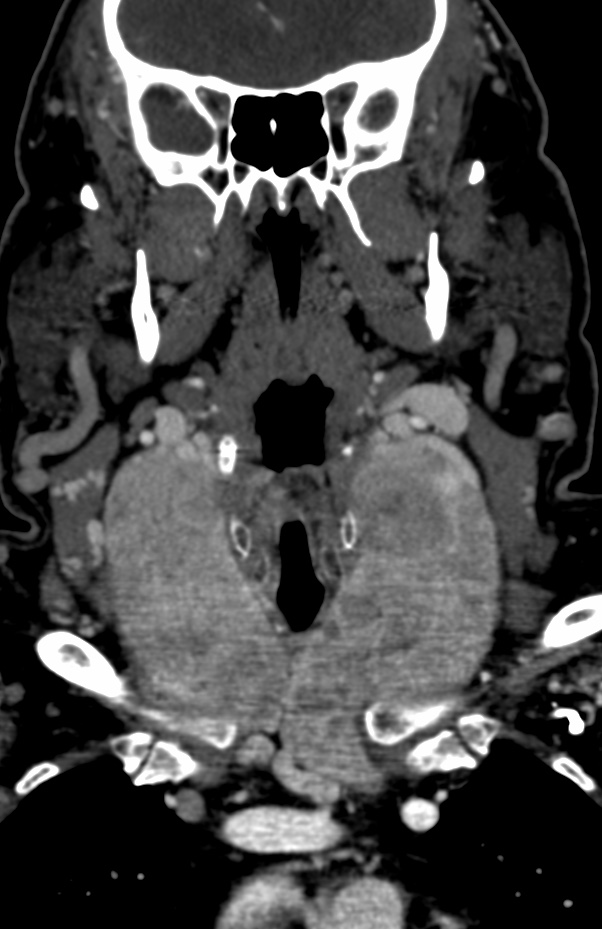
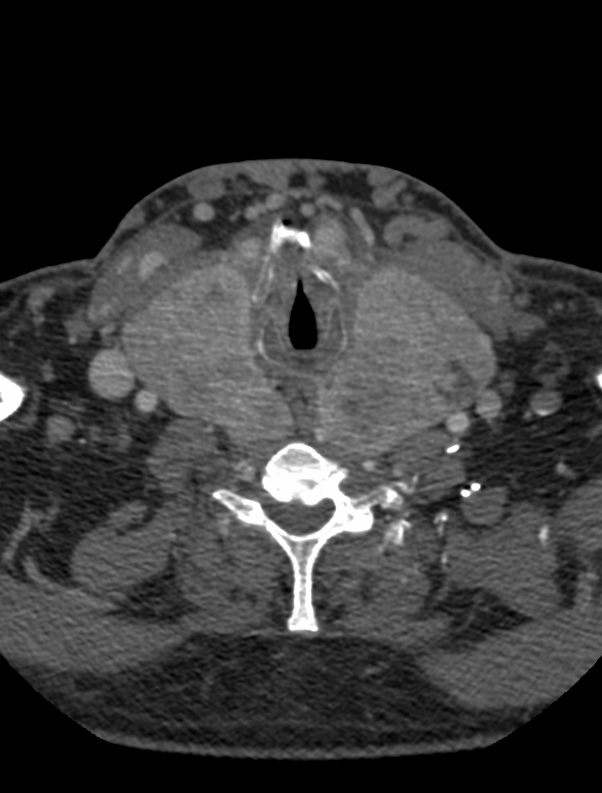
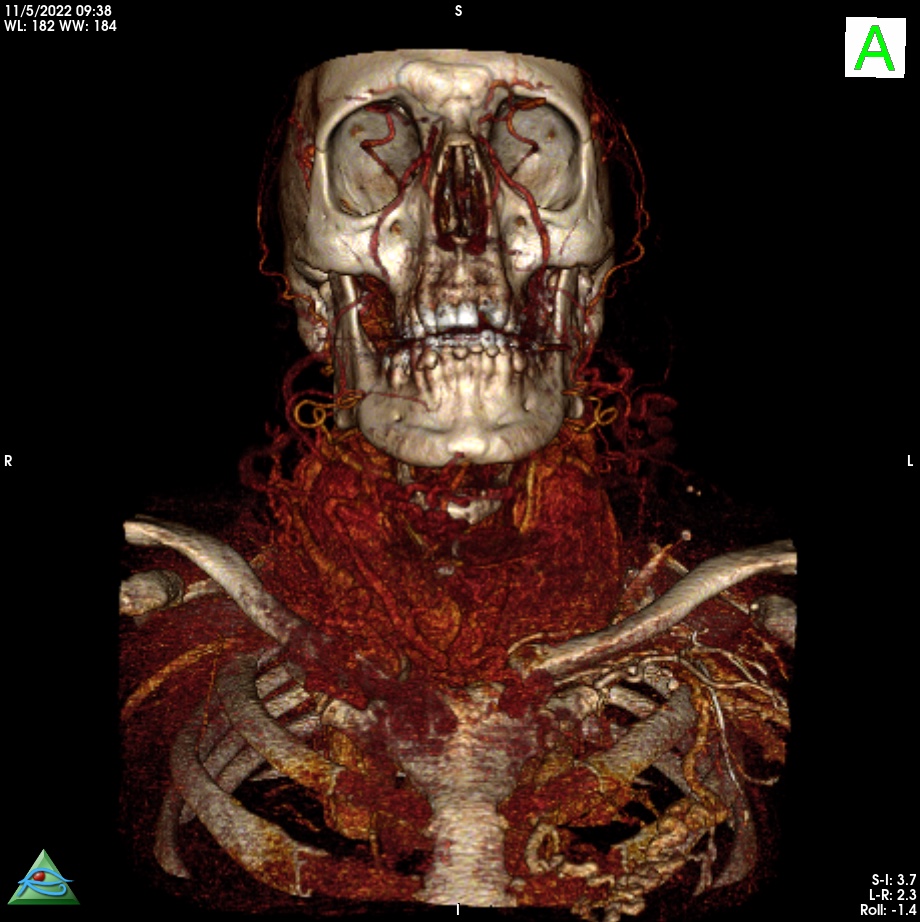
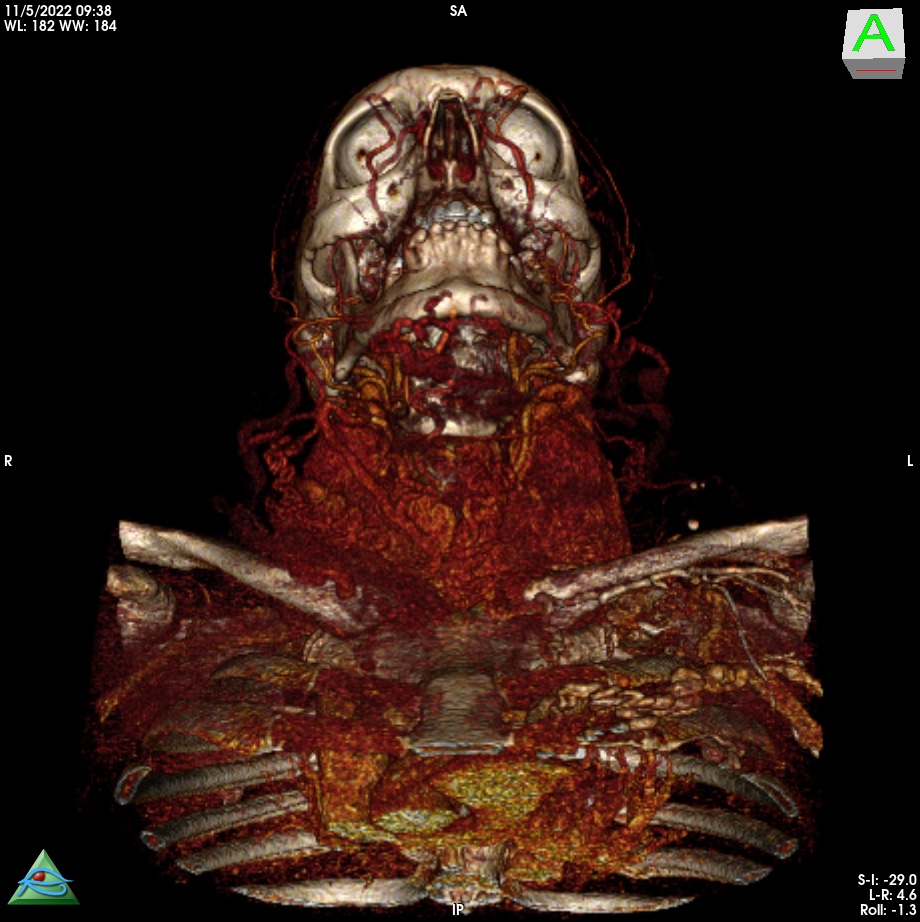
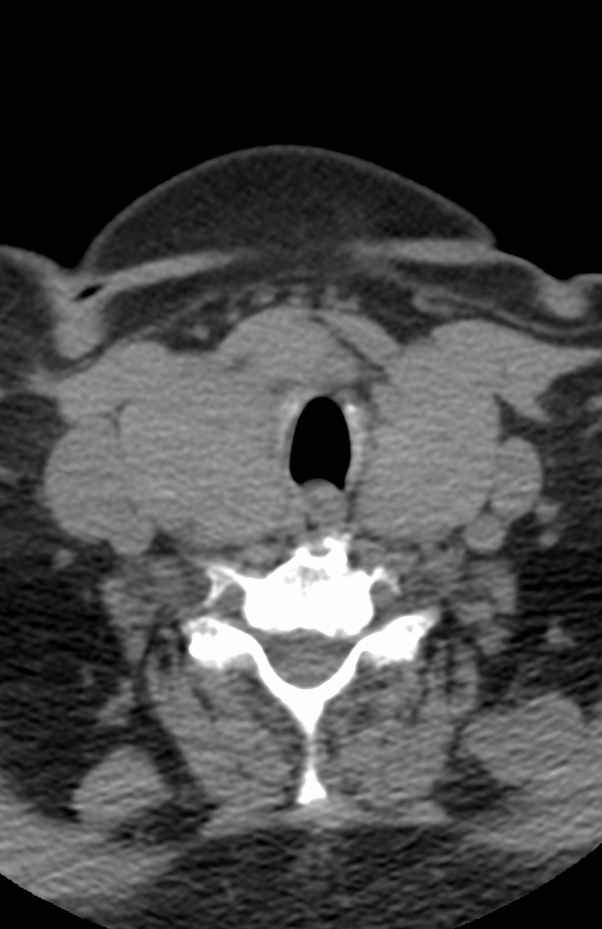
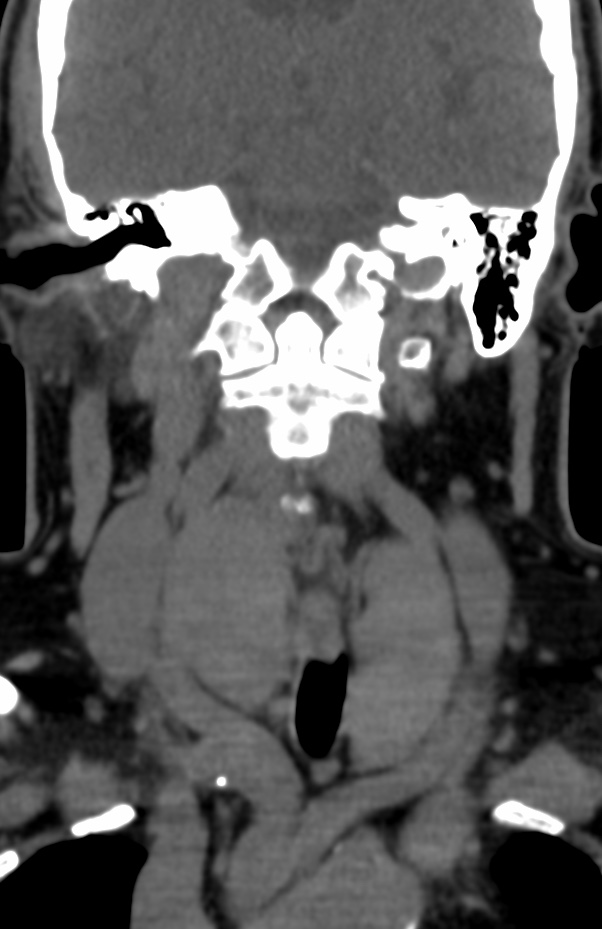
Anterior Versus Posterior: Most intrathoracic goiters lie anterior to the recurrent laryngeal nerve and anterolateral to the trachea. Goiters in the anterior mediastinum arise secondarily from the isthmus or the lower aspects of the thyroid lobes. As the mass grows inferiorly, the great vessels may be displaced laterally, framing the mass on chest radiography Posterior mediastinal goiters arise as secondary goiters from the posterolateral aspects of the thyroid gland and descend posterior to the great vessels. Most are right- sided because of anatomic barriers formed by the aortic arch and its branch vessels. Even goiters that originate from the left lobe are deflected to the right by the left innominate vein and left common carotid and subclavian arteries. The esophagus may be markedly displaced to the contralateral side and the trachea may be pushed anteriorly.
The goiter descends inferiorly along the fascial planes of the neck, following a path of least resistance into the superior mediastinum
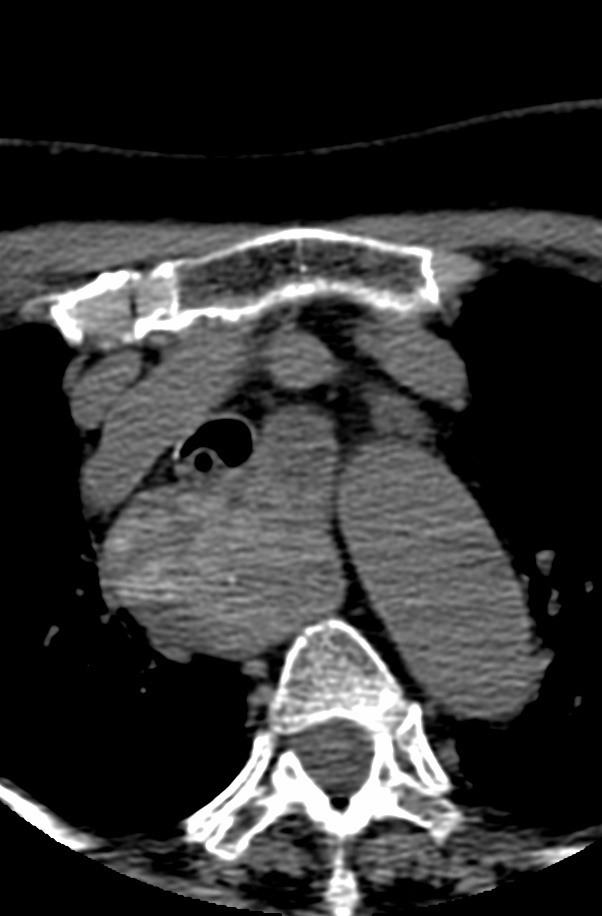

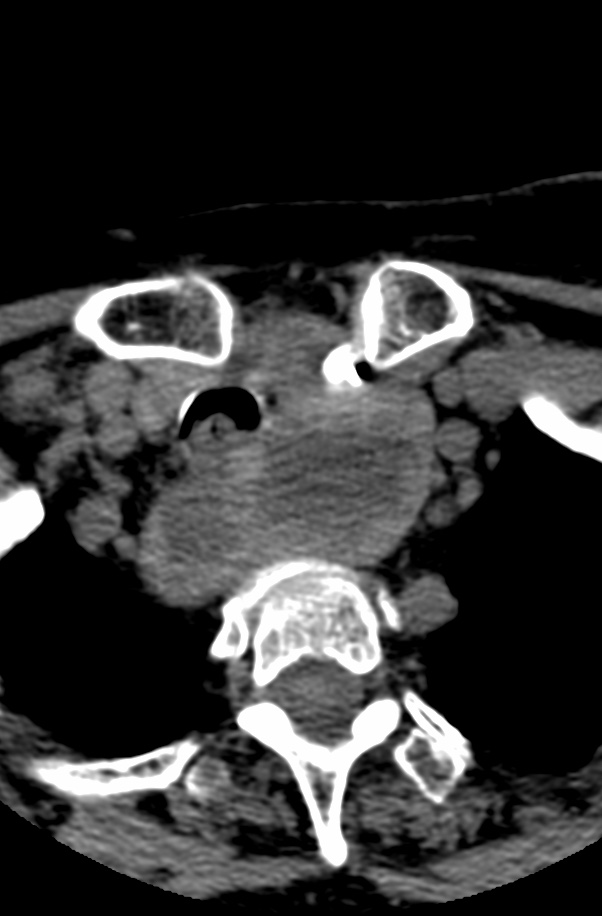
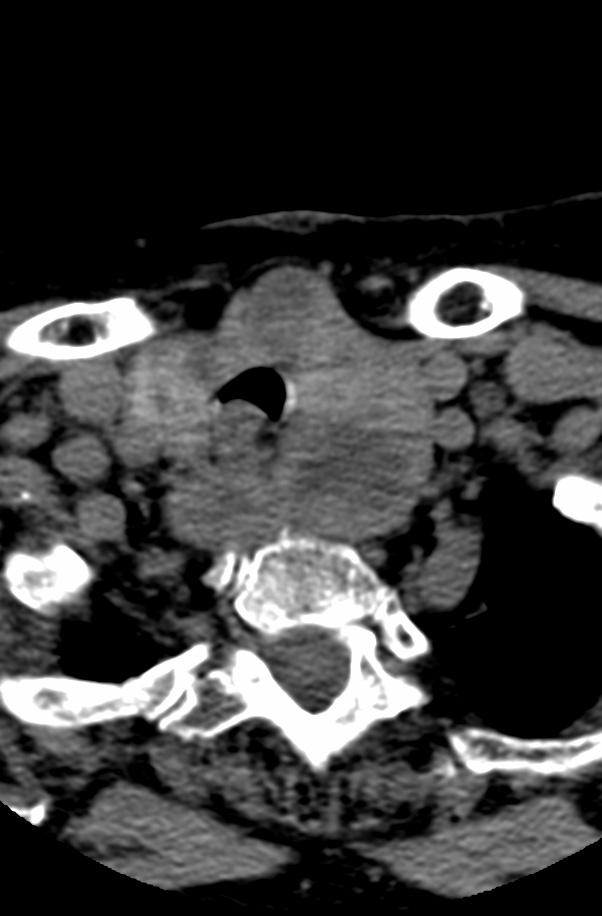
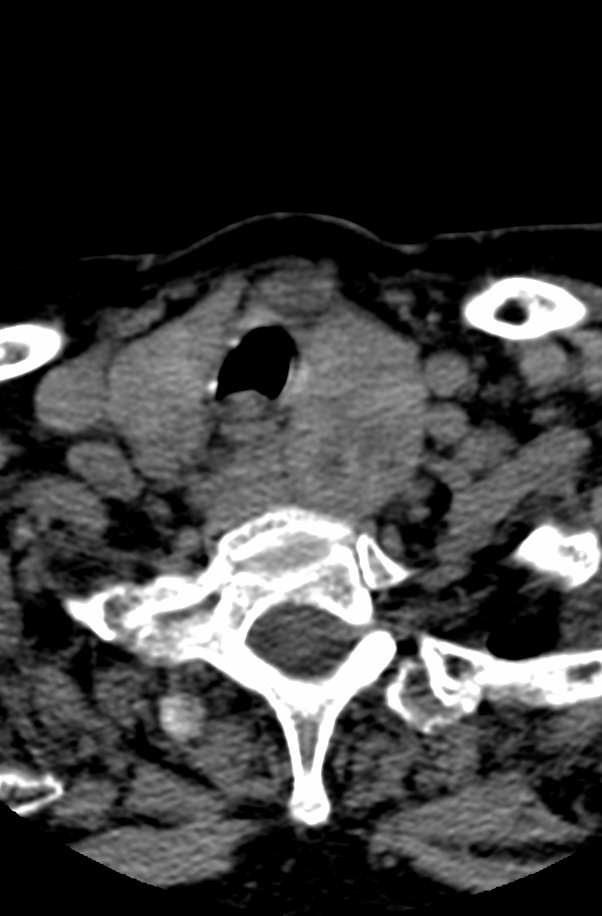
Although most patients are asymptomatic, stridor due to tracheal compression is the most common symptom . Findings include a sharply marginated mediastinal mass with punctate calcifications.
The differential diagnosis includes calcified lymph nodes. treated lymphoma. and a hemorrhagic primary mediastinal mass.



Reference:
AJR 1999;173:471-475 0361-803X/99/1732-471