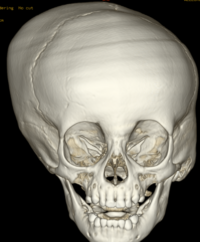
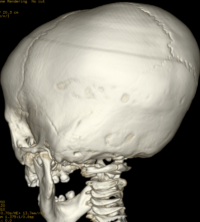


Craniosynostosis refers to the premature closure of the cranial sutures. The skull shape then undergoes characteristic changes depending on which sutures close early. 3D CT MIP can depict suture patency, extent of synostosis (ie, complete versus incomplete bone bridging), fracture extent and conspicuity, and three-dimensional calvarial deformity as a single set of projections in children with suspected craniosynostosis or skull fracture.
Types of craniosynostosis
There are several types of craniosynostosis. Most involve the fusion of a single cranial suture. Some complex forms of craniosynostosis involve the fusion of multiple sutures. Most cases of multiple suture craniosynostosis are linked to genetic syndromes and are called syndromic craniosynostosis.
The term given to each type of craniosynostosis depends on what sutures are affected. Types of craniosynostosis include:
- Sagittal (scaphocephaly). Premature fusion of the sagittal suture that runs from the front to the back at the top of the skull forces the head to grow long and narrow. Sagittal craniosynostosis results in a head shape called scaphocephaly and is the most common type of craniosynostosis.
- Coronal. Premature fusion of one of the coronal sutures (unicoronal) that run from each ear to the top of the skull may cause the forehead to flatten on the affected side and bulge on the unaffected side. It also leads to turning of the nose and a raised eye socket on the affected side. When both coronal sutures fuse prematurely (bicoronal), the head has a short and wide appearance, often with the forehead tilted forward.
- Metopic. The metopic suture runs from the top of the bridge of the nose up through the midline of the forehead to the anterior fontanel and the sagittal suture. Premature fusion gives the forehead a triangular appearance and widens the back part of the head. This is also called trigonocephaly.
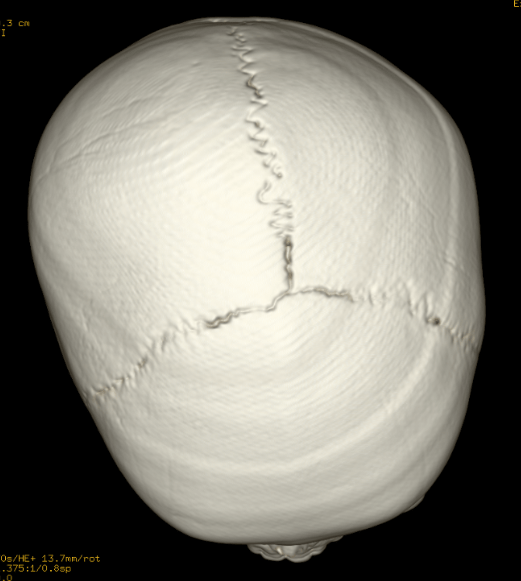
- Lambdoid. Lambdoid synostosis is a rare type of craniosynostosis that involves the lambdoid suture, which runs along the back of the head. It may cause one side of your baby’s head to appear flat, one ear to be higher than the other ear and tilting of the top of the head to one side.
Ref; Robertson RL, Ball Jr, WS, Barnes PD. Skull and brain. In: Kirks DR, Griscom NT, eds. Practical Pediatric Imaging: Diagnostic Radiology of Infants and Children, 3rd ed. Philadelphia: Lippincott-Raven; 1998:65-200
AJNR 2000, 21 (10) 1951-1954;