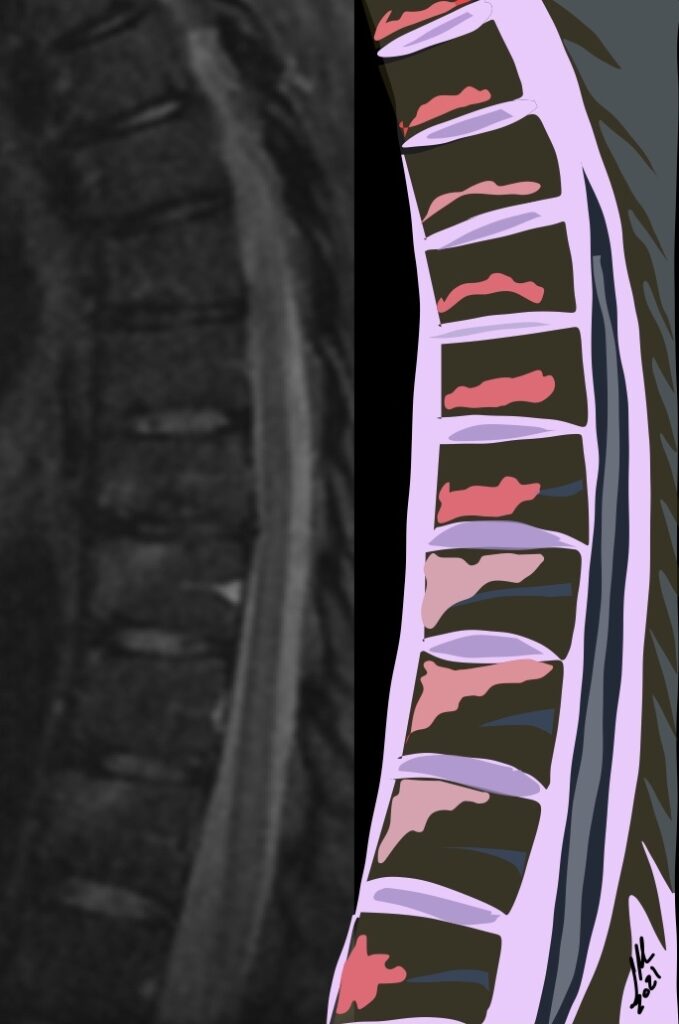
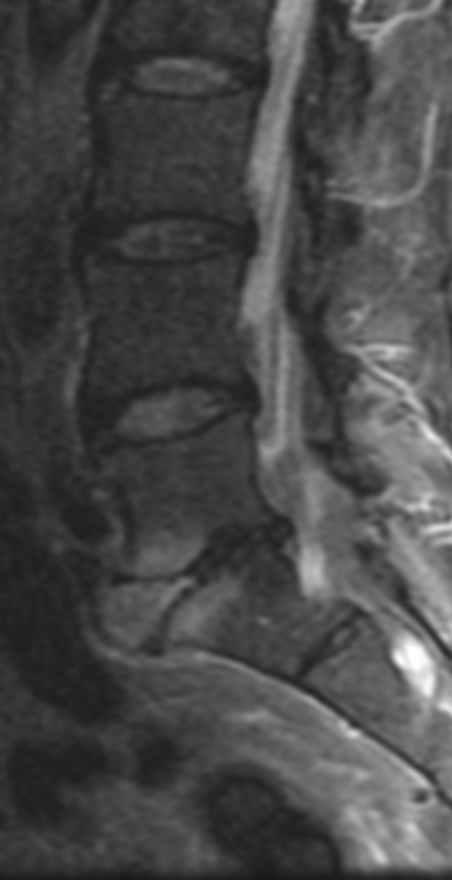
AL are characterized by high signal intensity at the cortical plates adjacent to intervertebral disks on STIR images and T1+C FAT SAT. High signal intensity may also be visible in the center or throughout the intervertebral space, simulating inflammatory diskitis. Andersson lesions are observed in 33% of patients with spondyloarthritis, and this finding has a specificity of 59% for this group of diseases
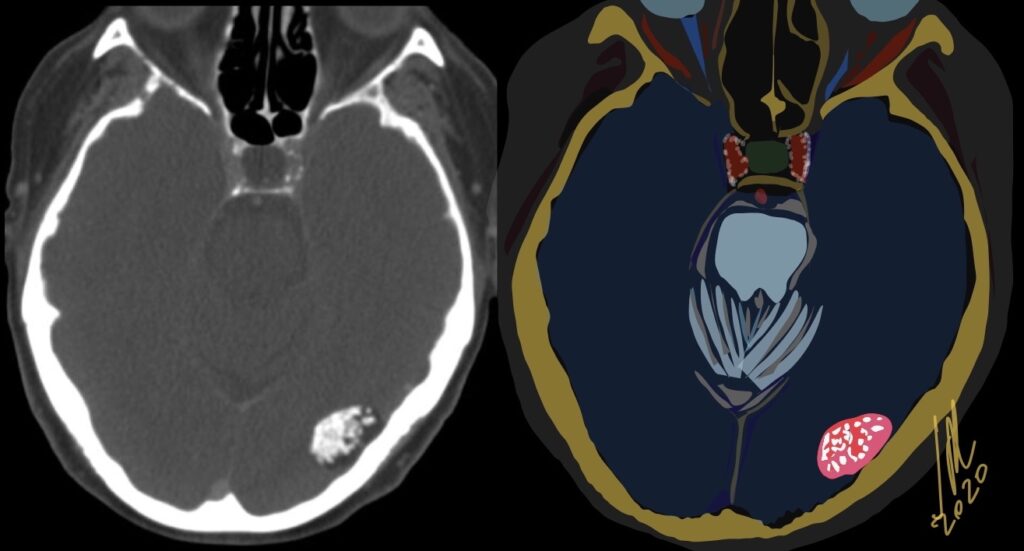
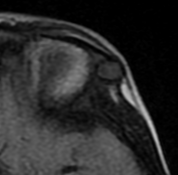
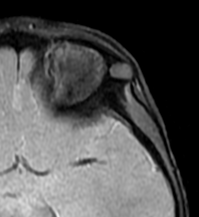
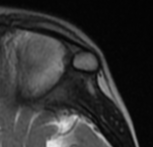
Epidermoid cysts have a thin squamous lining, which only rarely contains calcifications. These cysts contain debris from the desquamation of their squamous epithelial lining. The debris consists of mostly keratin, a proteinaceous material, and some cholesterol, a lipid material derived from the breakdown of cell membranes. On CT, the epidermoid cysts appeared hypodense with no evidence of enhancement after contrast material and edema is absent. 1.5% located in Cerebral hemispheres and 25% are calcified.
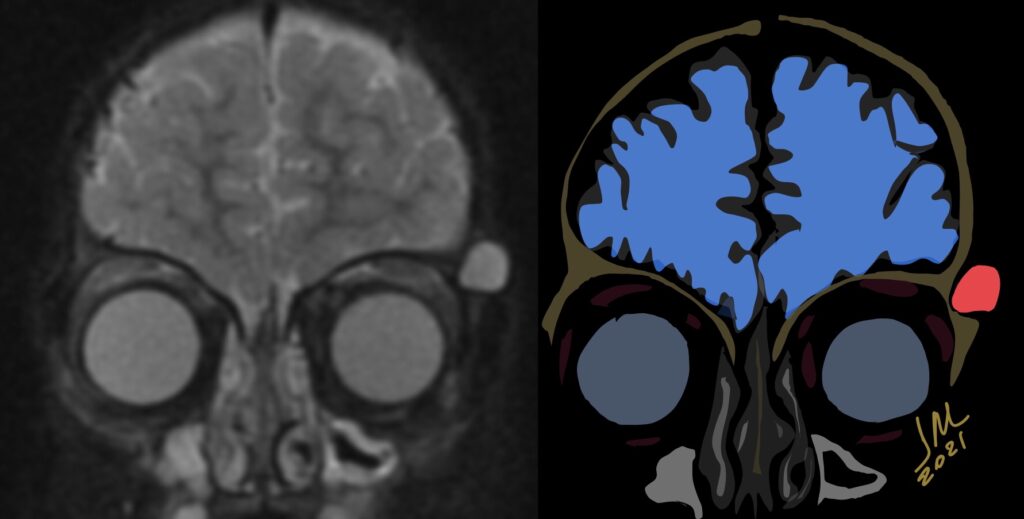
10% of intracranial epidermoids are extradural, being encountered most often in the skull as intradiploic masses in the temporal, occipital, parietal and frontal bones. Most manifest as painless, visible masses and are usually found along the lines of embryologic fusion; the zygomaticofrontal and the frontoethmoidal sutures
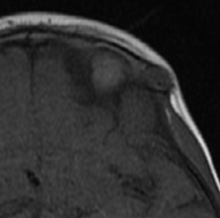
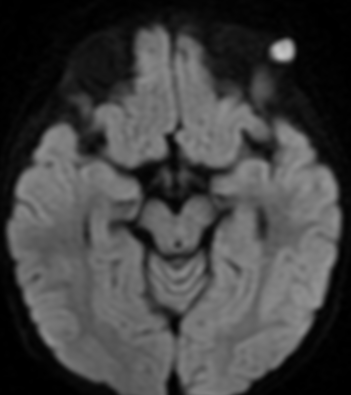
On MRI, epidermoids are hypointense on T1 hyperintense on T2 and maybe the most important thing have high signal intensity on DWI.
Differential diagnoses include dermoid cysts, eosinophilic granulomas, cholesterol granulomas, hemangiomas, aneurysmal bone cysts, fibrous dysplasia and eosinophilic granuloma.
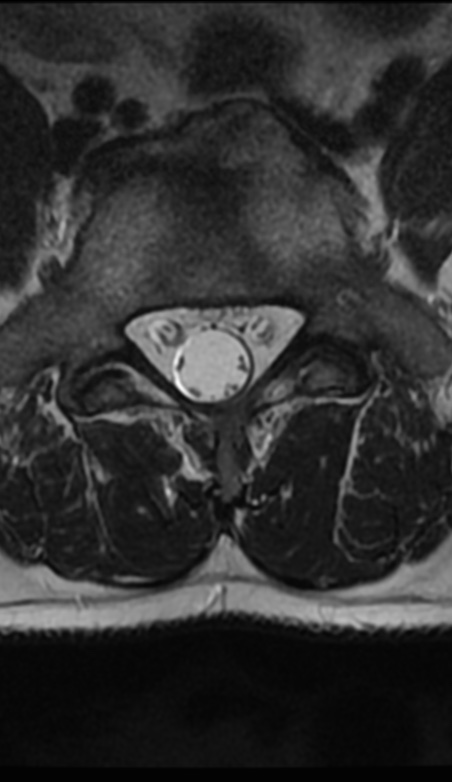
Could be important to consider the possibility of discogenic visceral pain secondary to anterior herniation of the lumbar disc when forming a differential diagnosis for seemingly idiopathic abdominal pain. Visceral pain is a very frequent cause for medical consulting. Afferent fibers innervating viscera project to the central nervous system via sympathetic nerves. The lumbar sympathetic nerve trunk lies in front of the lumbar spine. Thus, it is possible for patients to suffer visceral pain originating from sympathetic nerve irritation induced by anterior herniation of the lumbar disc.
The most important thing is that it is always a diagnosis of exclusion and highly questioned.
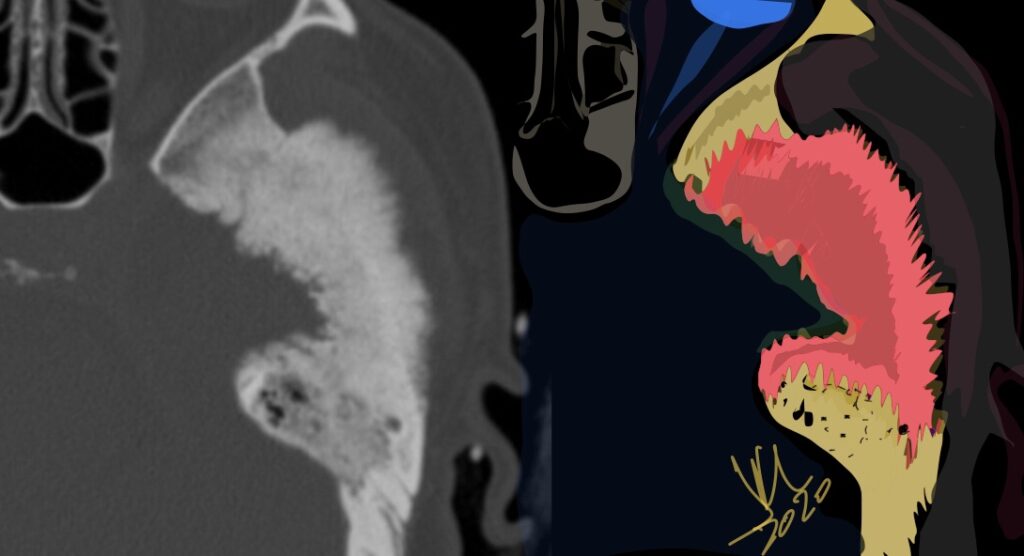
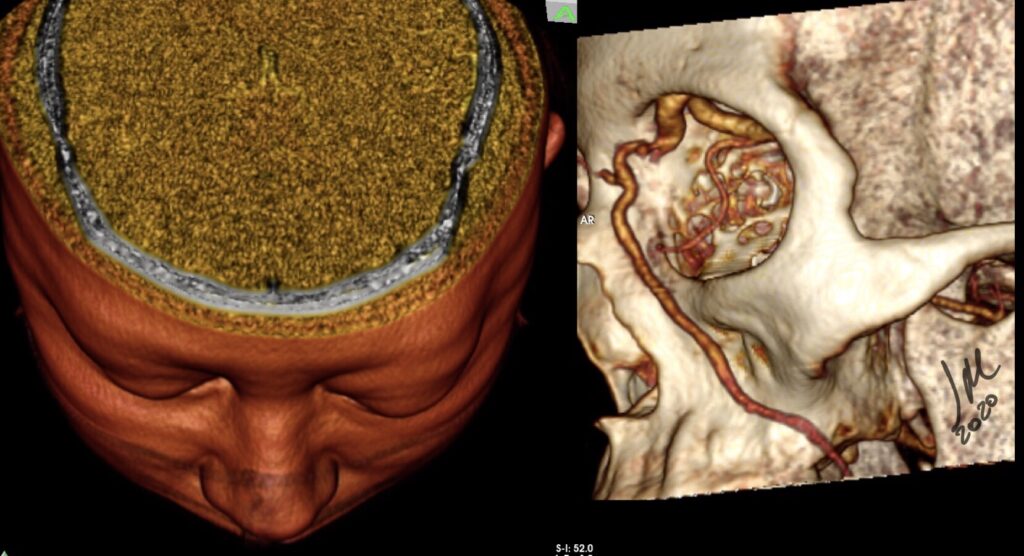
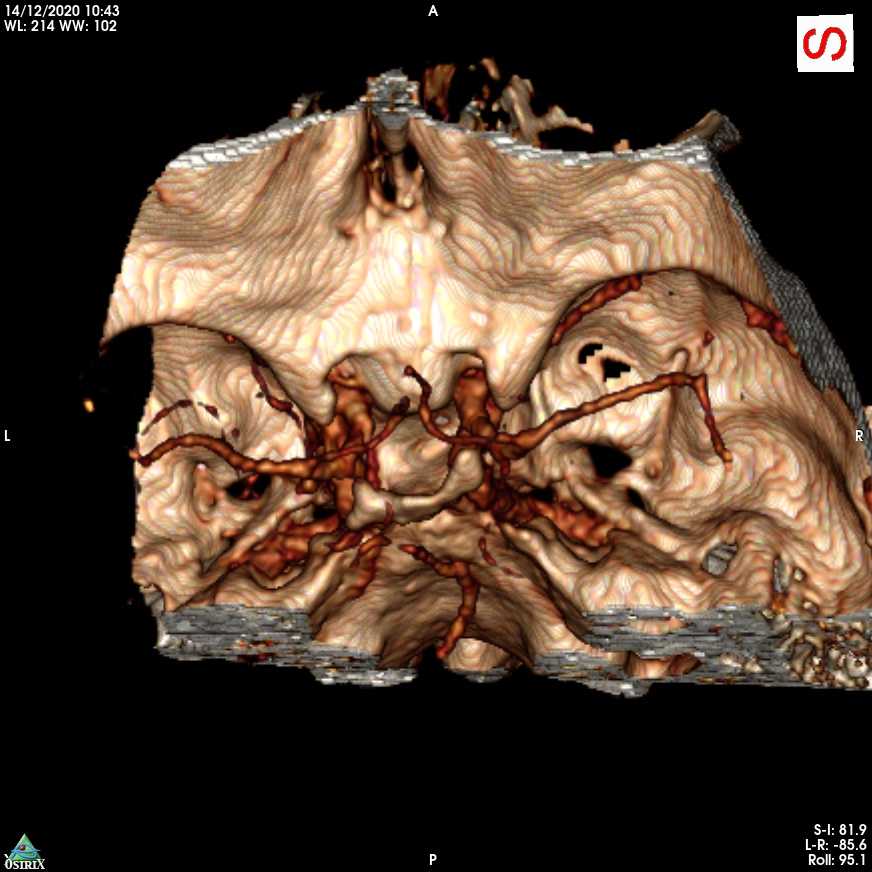
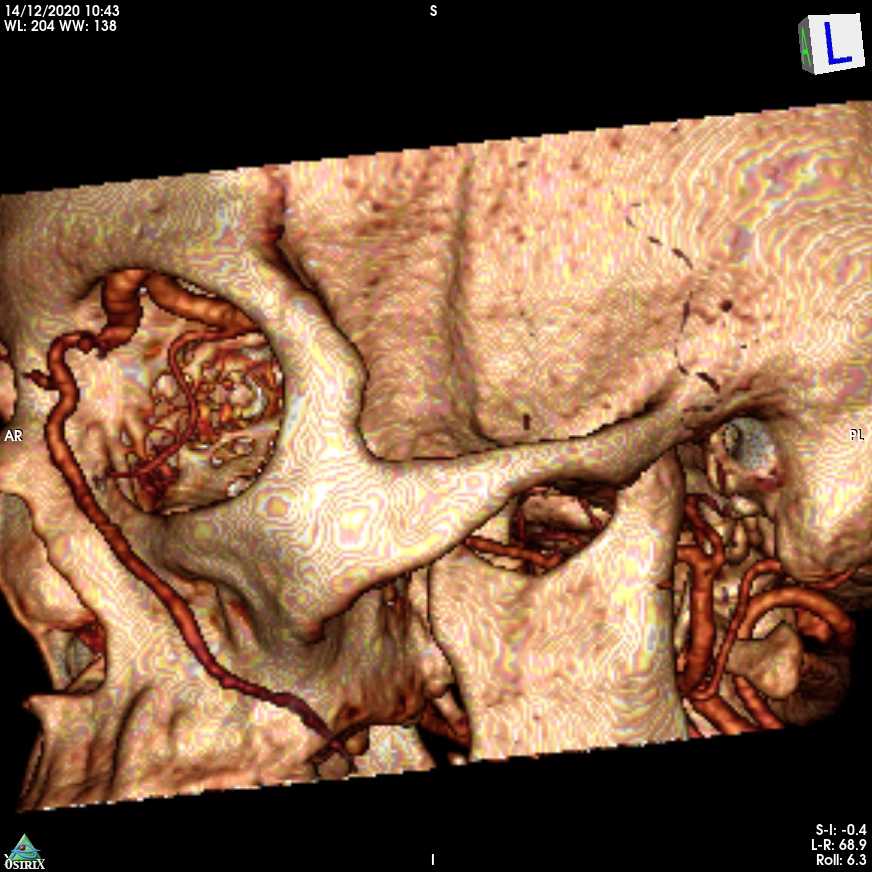
Meningioma primary to the tegmen tympani arise from the floor of the middle cranial fossa and spread inferomedially into the middle ear cavity.
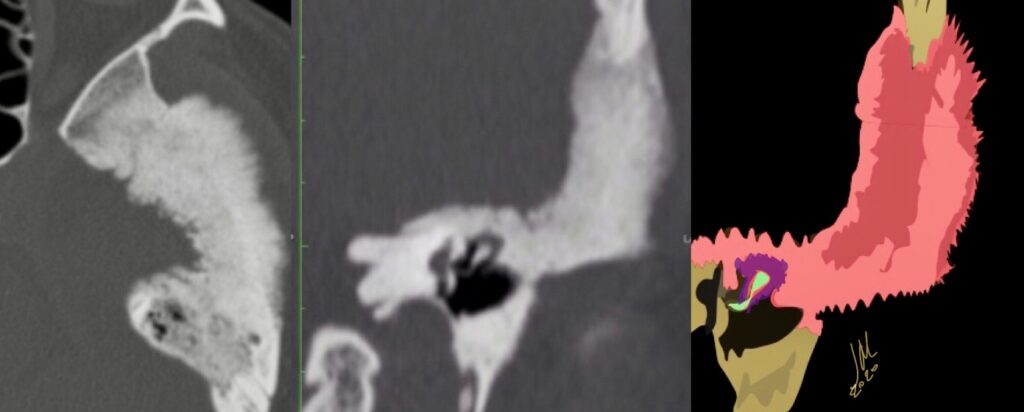
CT features included thickening of the tegmen tympani, The internal trabecular architecture of the involved bone is preserved (trabecular hyperostosis). The inner margin of the involved calvaria along the lateral aspect of the middle cranial fossa is irregular. A middle ear cavity soft-tissue mass resulted in ossicular encasement. There is no ossicular erosion or destruction. Facial nerve canal encroachment is present.
Tegmen tympani meningioma bone changes on CT can be confused with fibrous dysplasia of this area. Preservation of internal trabecular architecture distinguishes it from the ground-glass attenuation seen in typical fibrous dysplasia.
The other dominant consideration for tegmen tympani meningioma on CT is cholesteatoma; however, on CT, meningiomas lack the bone and ossicular destructive changes. These all lack the characteristic tegmen tympani thickening on CT and dural enhancement along the floor of the middle cranial fossa seen with meningioma on enhanced MR imaging. Enlargement of the facial canal typical of schwannoma is not seen with meningioma. Facial nerve hemangioma causes amorphous honeycomb bone changes on CT in larger lesions, which differ from the trabecular hyperostosis of tegmen tympani meningioma. Ossifying variants of hemangioma may have spicules of lamellar bone, which could more easily mimic meningioma on CT; however, most facial nerve hemangiomas are primarily centered in the geniculate fossa. This location should help distinguish them from meningioma
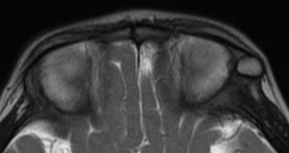
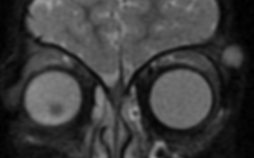
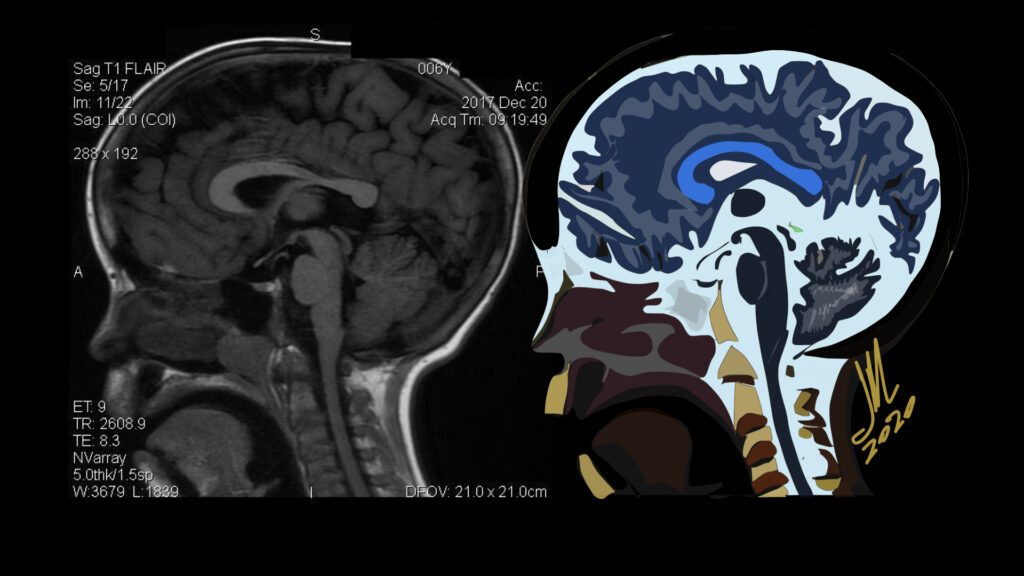
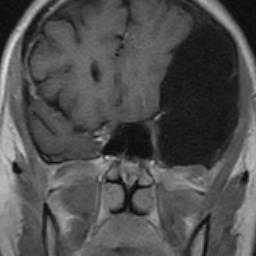
Characteristic maxillofacial findings of acromegaly include thickening of the calvaria, more pronounced in the inner table, enlarged paranasal sinuses, most often the frontal sinus, resulting in frontal bossing, and enlargement of the mandible, which may lead to prognathism and gaps between the teeth. Diffuse and symmetric enlargement of the extraocular muscles has been described as part of the generalized organomegaly associated with acromegaly.
Successful surgical treatment of functional pituitary microadenoma largely relies on accurate identification of the tumor within the sella turcica.These relatively small tumors represent a challenge to both neuroradiologists and neurosurgeons in locating them, resulting in a greater potential for insufficient treatment of the lesion.
The criterion standard technique used for lesion localization is MR imaging. Dynamic contrast-enhanced technique is often applied on MR imaging to overcome this issue, scanning time usually required to obtain each dynamic phase ranges from 20 to 30 seconds or is shortened into 12–20 seconds in some cases, but it is not possible to obtain a gapless 3D image. The most suitable time phase to obtain sufficient contrast between an adenoma and the normal pituitary gland is 45–60 seconds after contrast agent injection. This adenoma-normal pituitary gland contrast will rapidly diminish within the subsequent 30 seconds. Both spatial and temporal resolution must, therefore, be sufficiently high to visualize the presence of the adenoma.
Acromegaly results from excessive production of growth hormone, most commonly in patients with pituitary adenoma >95% of cases, resulting in the overproduction of insulinlike growth factor 1. Acromegaly is a multisystem disease characterized by somatic overgrowth of osseous structures such as the hands, feet, skull, mandible, and nose. Soft-tissue thickening of the skin and vocal cords and enlargement of internal organs including the heart and kidneys also can be seen. Overproduction of growth hormone before epiphyseal closure leads to linear overgrowth and gigantism
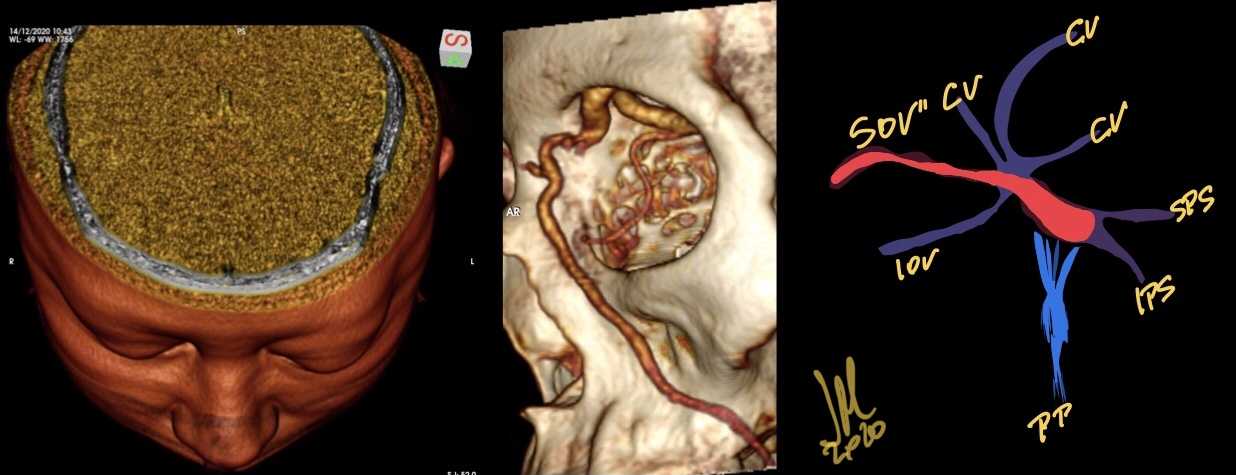
Pulsating exophthalmos, bruit, and conjunctival chemosis have long been regarded as the three classical symptoms of carotid cavernous fistula. If the main venous drainage is via the superior ophthalmic vein, this triad will probably be present; if not, the triad is likely to be absent or incomplete.
The symptoms of patients with spontaneous CCF are commonly milder than those in traumatic CCF cases. This difference is attributable to the difference in the volume of blood flow into the cavernous sinus. In addition, the specific venous drainage from the cavernous sinus is important.
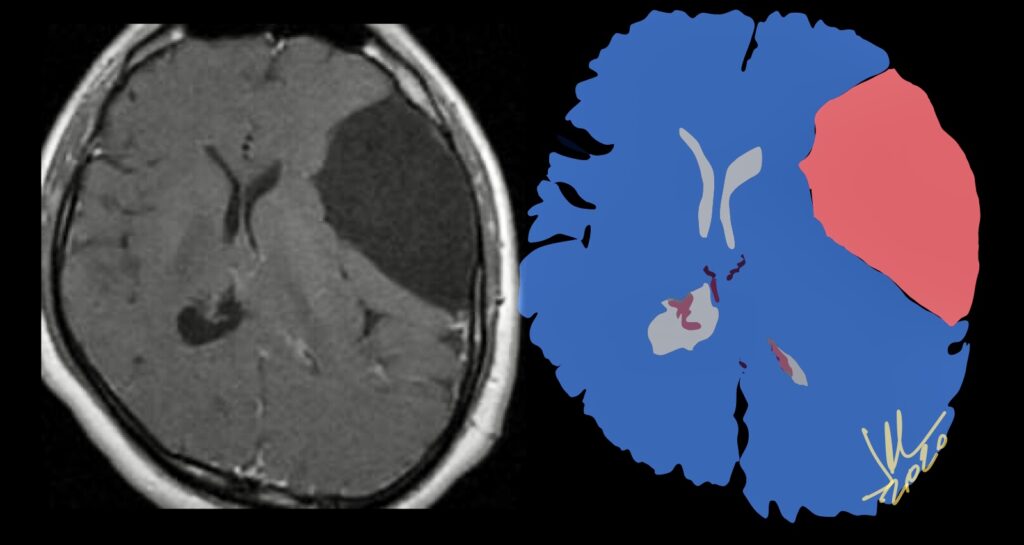
GALASSI CLASSIFICATION OF MIDDLE TEMPORAL FOSSA IACS
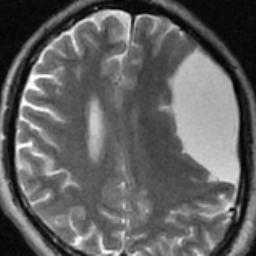
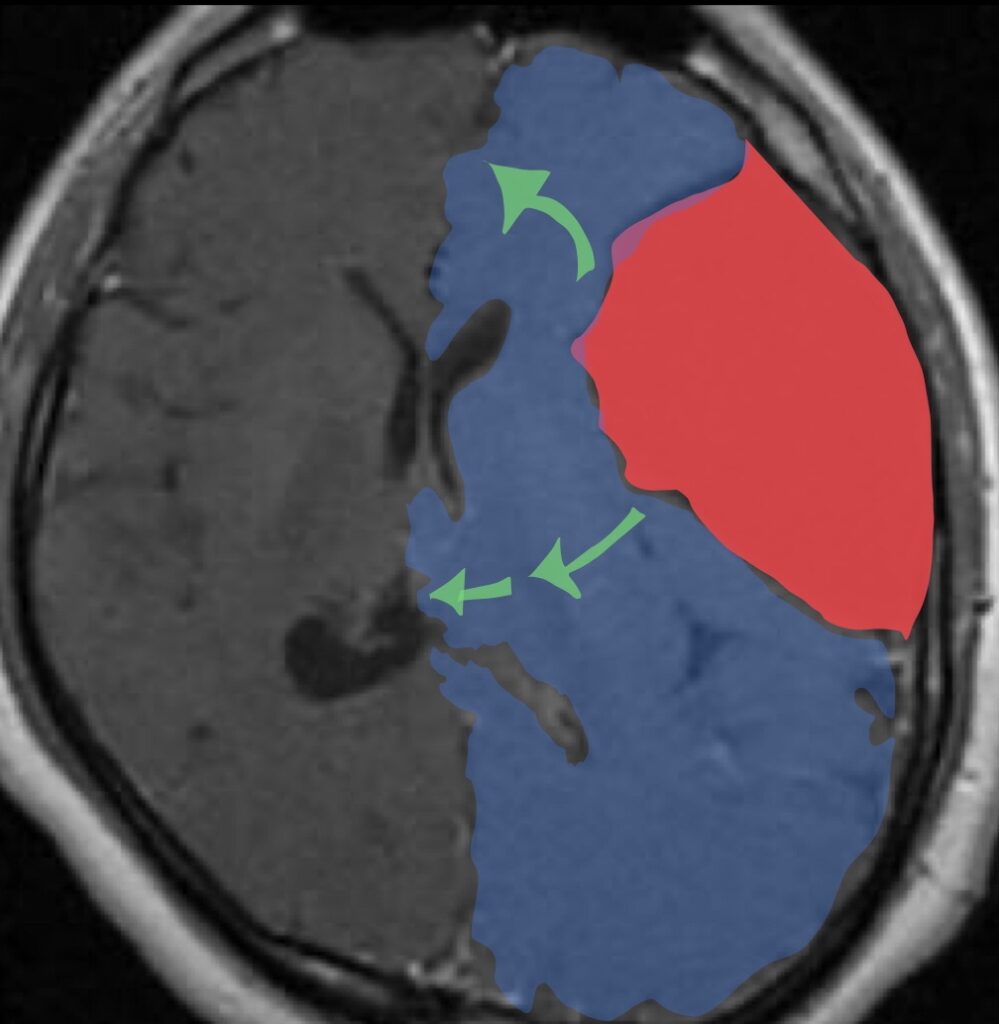
MTF ACs account for more than half of all ACs . The widely used Galassi Classification (1982) provides a schematic radiological classification of these lesions. There are three types of MTF IACs based on size and degree of mass effect.
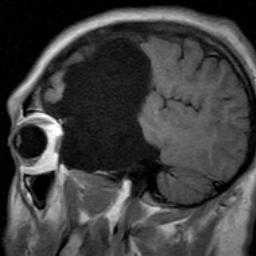
Type I cysts are characterized by the following: lens-shaped, anterior tip of the MTF, freely communicate with CSF/surrounding subarachnoid space on MR-cine/CT-ventriculography, they rarely require surgery.
Type II cysts are characterized by intermediate size, more rectangular morphology, extend into the Sylvian fissure, have variable communication with CSF pathways, and exert local mass effect on the temporal lobe; they occasionally and sometimes require surgery.
Type III cysts constitute the largest group, extend the full length of the Sylvian fissure, exert significant mass effect (often with midline shift), and do not communicate with the subarachnoid space; these usually require surgery.
There is no Class I evidence regarding the optimal treatment of ACs. We must, therefore, weigh the risks versus benefits of conservative versus surgical treatment of these lesions in symptomatic patients on an individual patient basis.
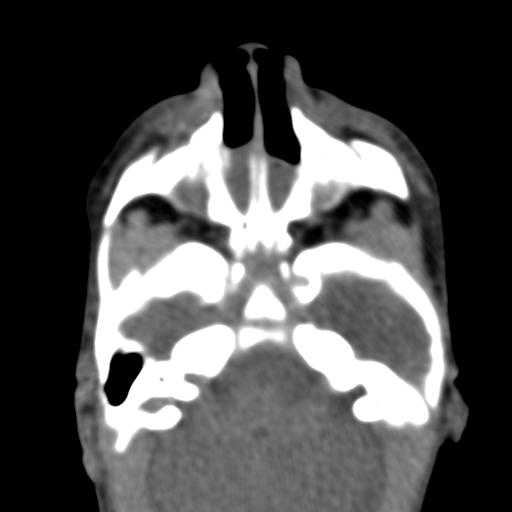
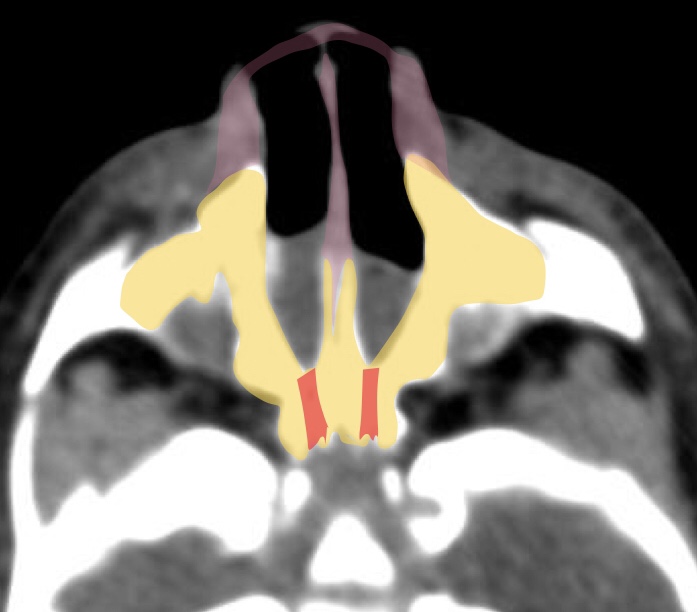
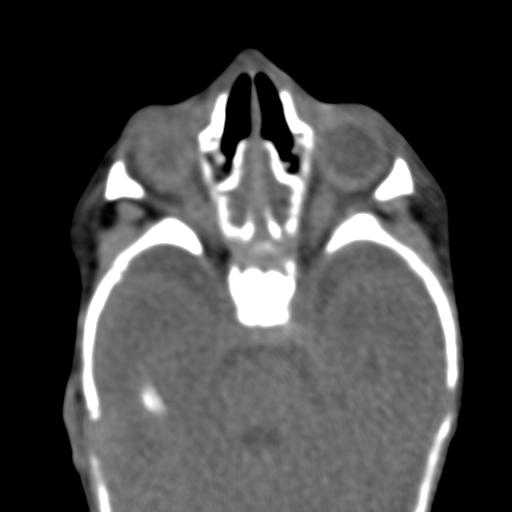
Choanal atresia is an uncommon developmental defect characterized by lack of communication between the nasal cavity and the nasopharynx. This plate may be bony (70-90%), membranous (10%), or both. The atresia may involve one or both nasal cavities, and other congenital anomalies may be associated with it. If bilateral choanal atresia is present at birth, it requires immediate diagnosis and intervention to permit respiration. Unilateral choanal atresia is usually diagnosed at a later stage.
CT in the axial plane was extremely valuable in demonstrating choanal atresia. The configuration of the nasal cavity is displayed in its entire length and it is possible to visualize stenosis and septal deviation and to differentiate between the bony and membranous components.
Other congenital anomalies such as craniofacial cleft palate, Treacher Collins syndrome, and cardiovascular and abdominal malformations have been reported in 20%-50% of cases of choanal atresia
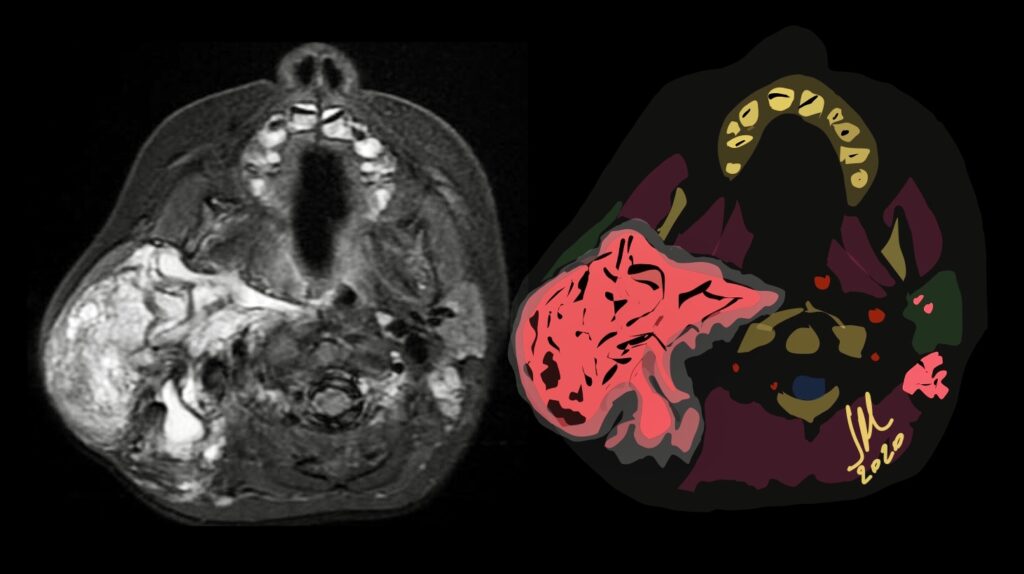
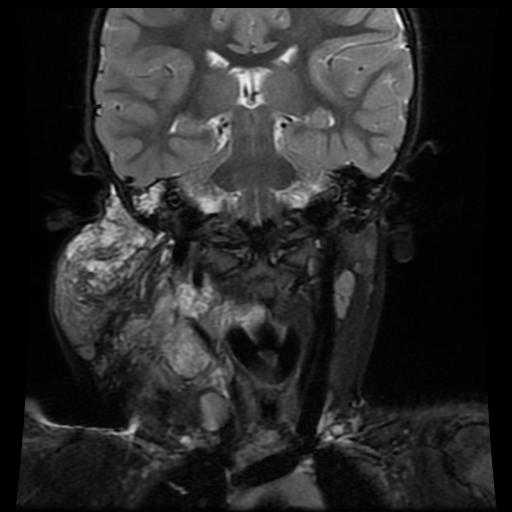
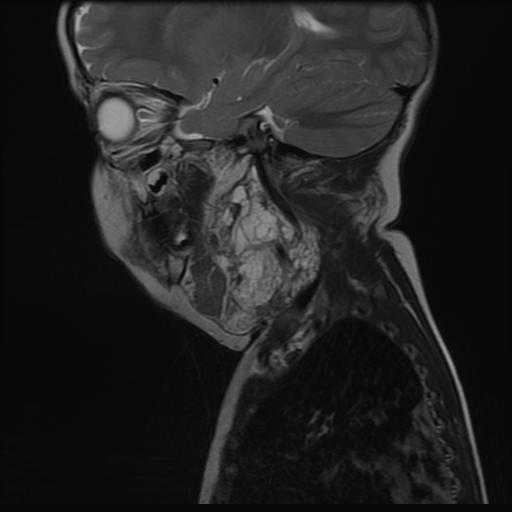
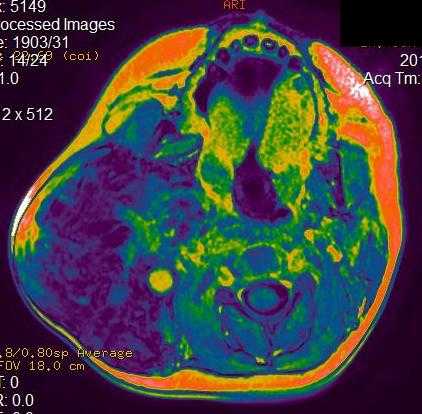
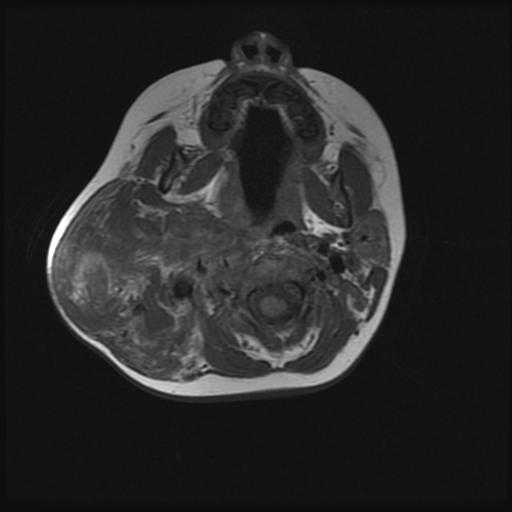
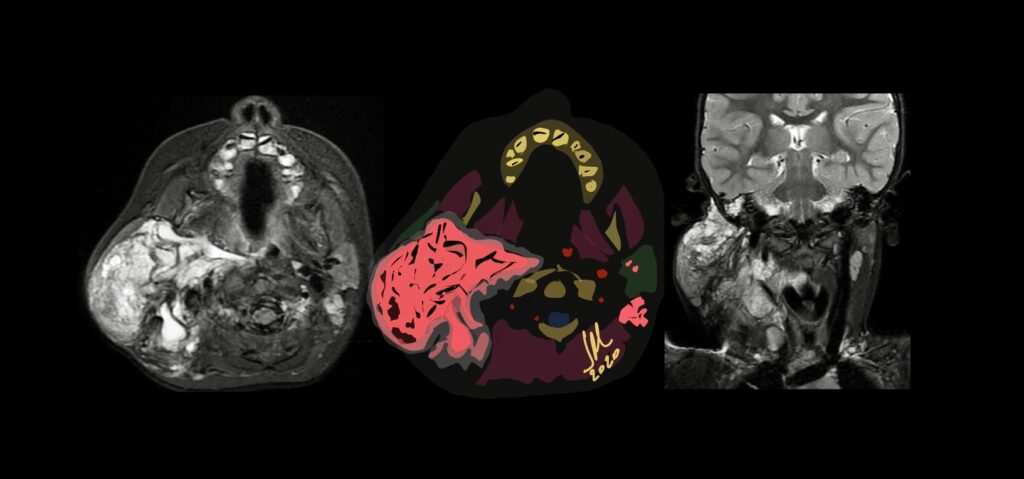
Lymphangiomas are rare congenital benign lesions occurring mainly in the head, neck and oral cavity frequently present at birth. Cystic hygromas, however, account for approximately 90% of the lymphangiomas in the head and neck region. Other common sites, outside the head and neck, include the axilla, shoulder, chest wall, mediastinum, abdominal wall, and thigh. They have no predilection for sex or race, and they have no malignant potential. Typical cystic hygromas cause no symptoms unless they enlarge in size or surround or invade adjacent normal anatomic structures. Cystic hygromas may cause symptoms such as feeding problems or breathing difficulties. Cystic hygromas are multilobulated, thin-wall, lymph-containing sacs. The fluid within the sacs is usually clear or amber colored, although occasionally it could be turbid or hemorrhagic.
MR imaging is useful to confirm the diagnosis and define the extension of the cystic lesions and their relationship to adjacent structures. A diagnostic dilemma may occur if a cystic hygroma containing a suspicious vascular anomaly is seen in the lower neck or upper mediastinum. In this case, the vascular malformation should be differentiated from a thoracic duct aneurysm.
They consist in localized centres of abnormal development of the lymphatic system. Three theories have been proposed to explain the origin of this abnormality. The first suggests that a blockage or arrest of normal growth of the primitive lymph channels occurs during embryogenesis, the second that the primitive lymphatic sac does not reach the venous system, while the third advances the hypothesis that, during embryogenesis, lymphatic tissue lays in the wrong area