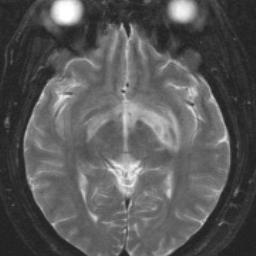
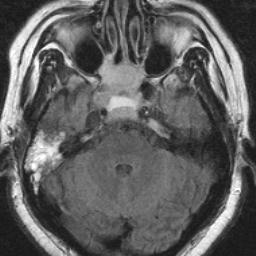
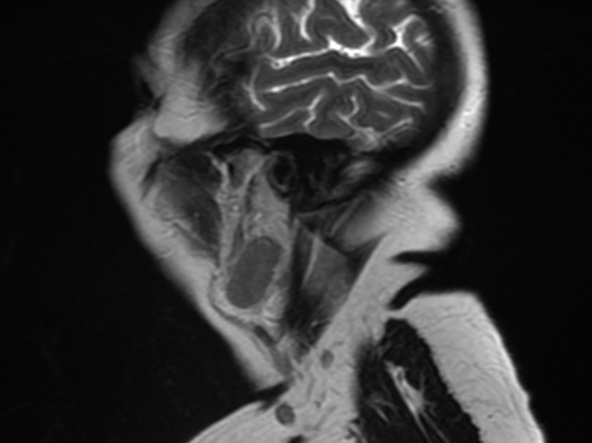
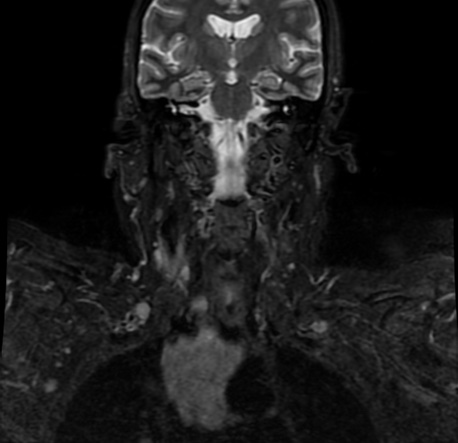
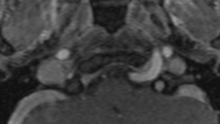
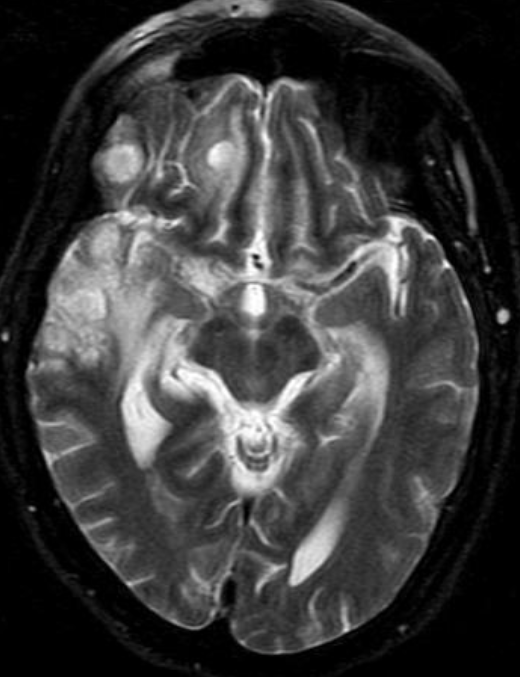
Themamillopontine distance or pontomamillary distance is defined as the distance between mamillary bodies to the superior aspect of the pons. When the mamillopontine distance is less than 5.5mm, it is an important indicator to diagnose intracranial hypotension.
Intracranial hypotension can be a challenging diagnosis because of the varied spectrum of clinical symptoms and is sometimes misdiagnosed as migraine headaches, meningitis, or a psychogenic disorder which can delay effective treatment.
the cause of intracranial hypotension may be identifiable, such as a sequela of trauma from skull base or facial fracture, craniospinal surgery, or lumbar puncture.
The clinical hallmark of intracranial hypotension is orthostatic headache.
Imaging is a critical part of identifying the diagnostic criteria for intracranial hypotension. There are five typical but variably present imaging characteristics: dural (pachymeningeal) enhancement, venous engorgement, pituitary hyperemia, subdural collections, and brainstem slumping.
Reference:
DOI:10.2214/AJR.12.8611 Intracranial Hypotension: Improved MRI Detection With Diagnostic Intracranial Angles
Rezaee, A., Smith, D. Mamillopontine distance. Reference article, Radiopaedia.org. (accessed on 31 Mar 2022) https://doi.org/10.53347/rID-43163
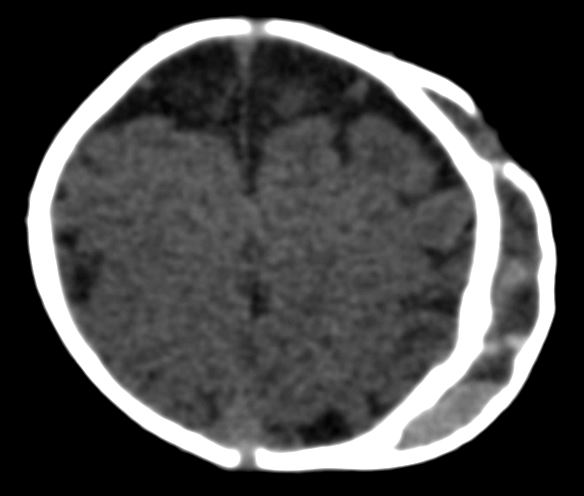
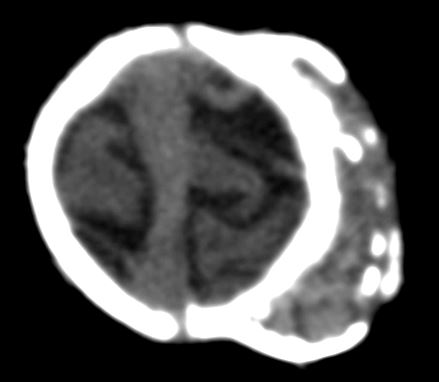
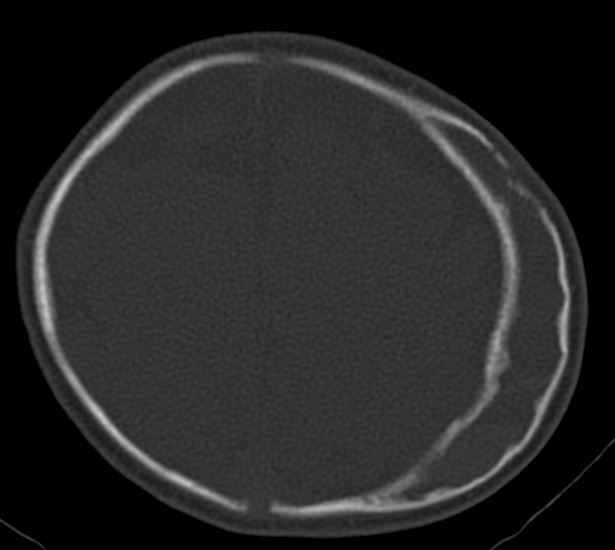
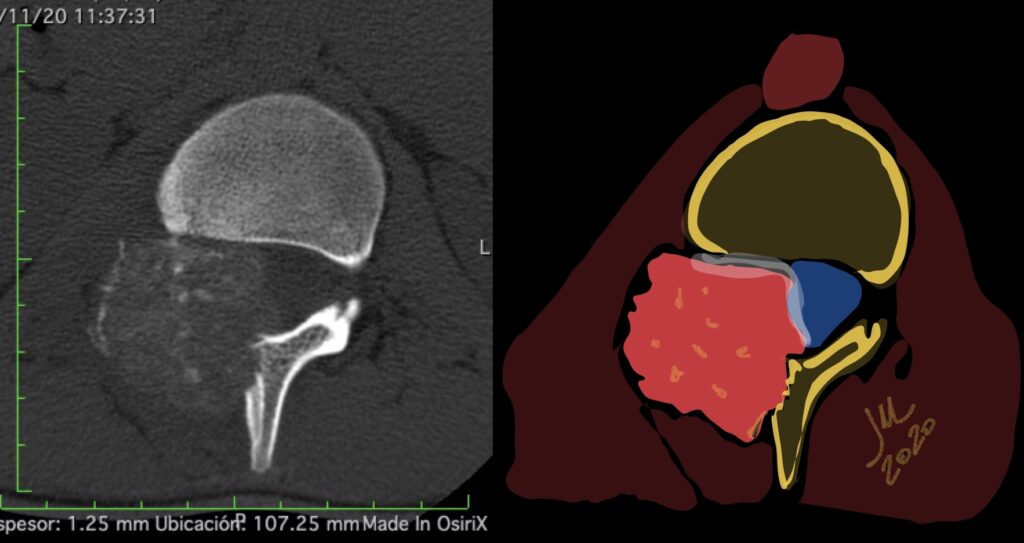
Calcified cephalohematoma of infancy is a result of a subperiosteal blood collection, that usually forms during birth-related trauma. It occurs when a cephalohematoma is not absorbed within the first weeks of its presentation and begins to ossify over the surface. The calcification may continue to enlarge. Calcification occurs in <5% of cephalohematomas.
Calcified cephalohematomas can permanently deform the infant cranium, and significant deformities often require correction. Although several reconstructive techniques have been proposed, there is no consensus on their management.
Images courtesy Dr. Andres Agudelo. Universidad Pontificia Bolivariana
Reference:
Management of Calcified Cephalohematoma of Infancy: A Single Institution 25-Year Experience University of Michigan – C. S. Mott Children’s Hospital, Ann Arbor, MI doi: 10.1097/01.GOX.0000720480.19319.a0
Al Kabbani, A., Bell, D. Calcified cephalohematoma. Reference article, Radiopaedia.org. (accessed on 30 Mar 2022) https://doi.org/10.53347/rID-72946
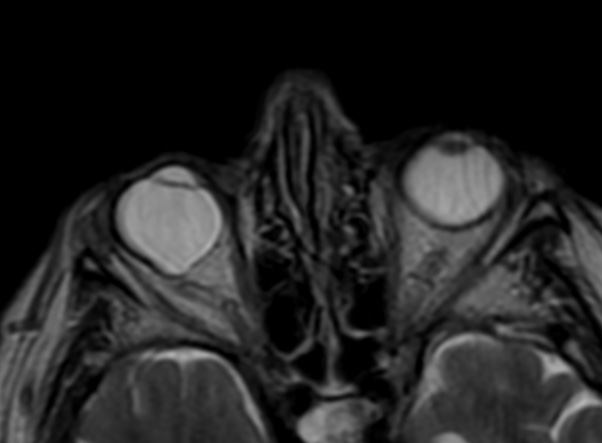
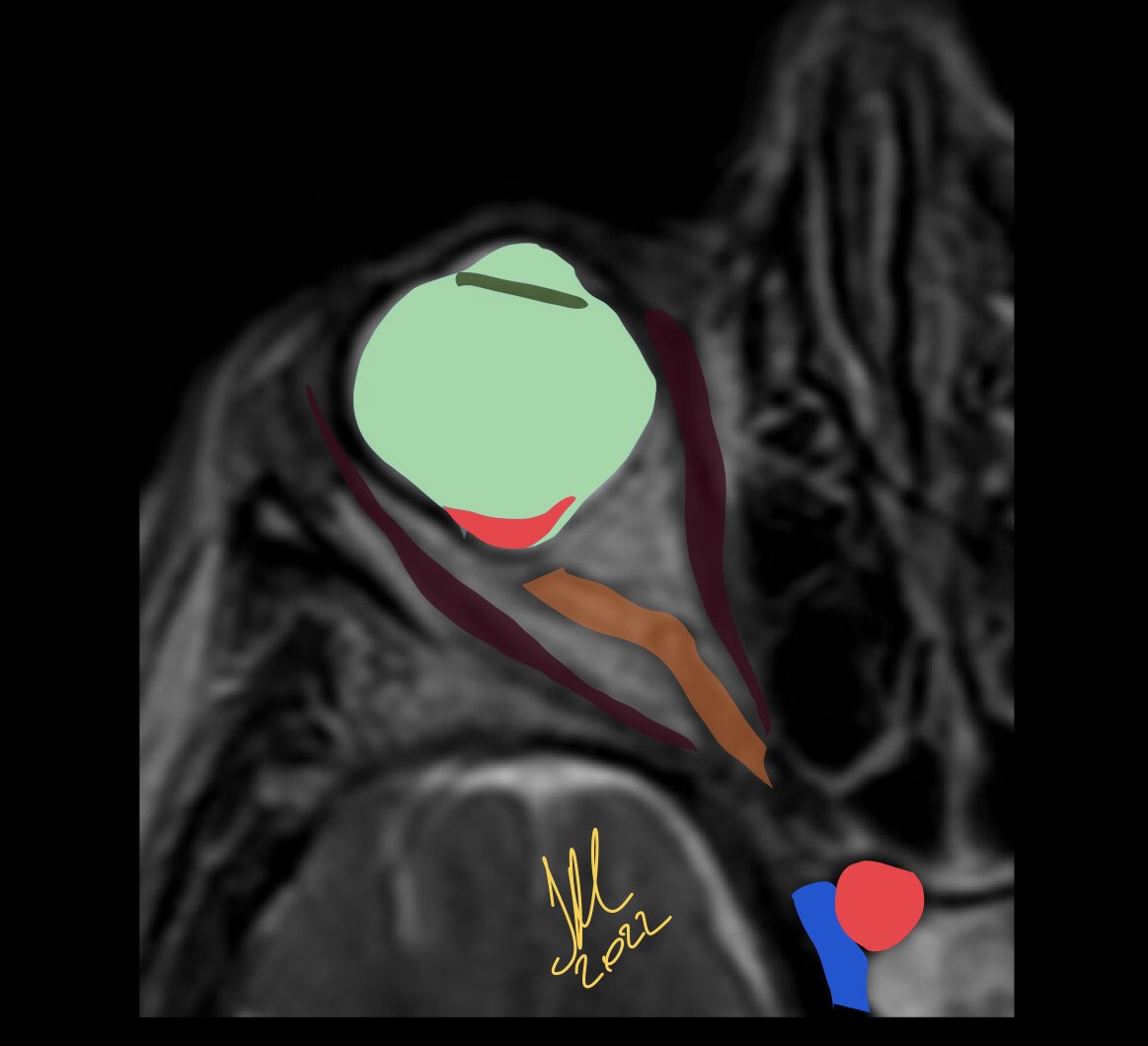
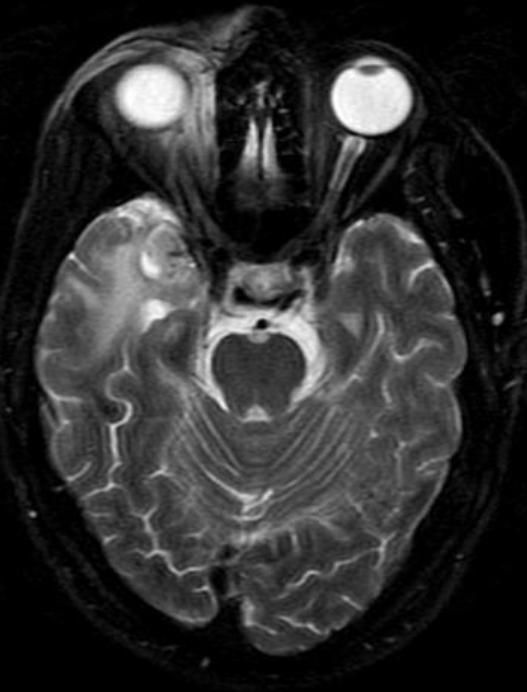
Posterior staphyloma is sine qua non of pathological myopia. It is characterized by disproportionate scleral ectasia with stretched conforming retinochoroidal layers. Conventionally, it has been classified into multiple types depending on location, although it usually involves the posterior pole of the eye. This outbulge, however, is a major risk factor for visually impairing maculopathy. PS can also be seen independent of high axial myopia.
As opposed to coloboma, staphyloma defect is located off-center from the optic disc, typically temporal to the disc.
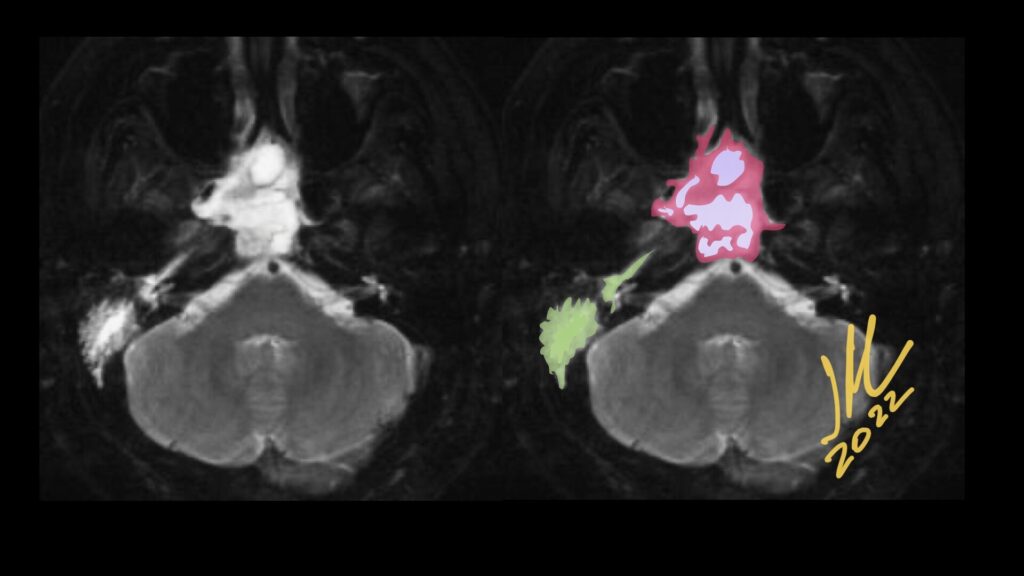
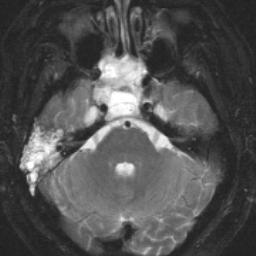
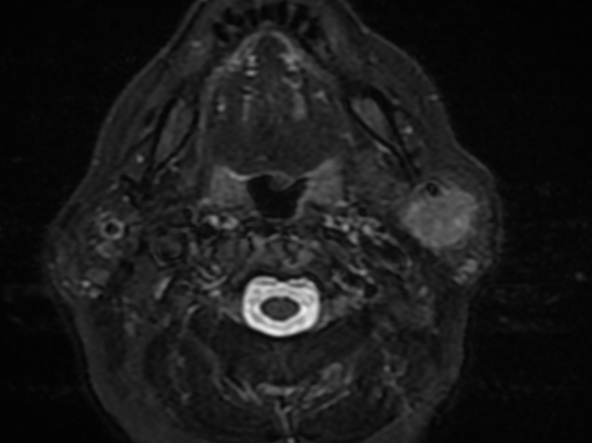
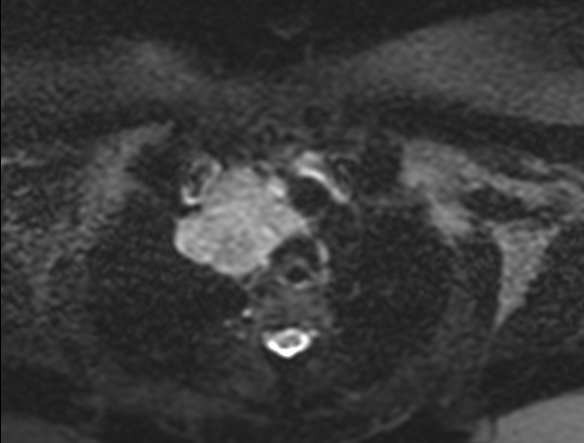
Primary nasopharyngeal adenoid cystic carcinoma (NACC), classified as a pathological type of adenocarcinoma, is a rare epithelioid malignancy that represents only 0.13% of all nasopharyngeal malignancies, but occurs most frequently in the salivary glands.
The main radiological characteristic is the tendency to perineural spread.
NACC lesions are located in the submucosal space of the pharyngonasal cavity without a well-defined boundary. Patients show masses with several obviously lobulated shapes, spreading along the interspaces around the cavity. the extension patterns and just characterized NACC as slow growth, frequent local recurrence, and metastatic spread.
the appearance in MR are isointense on T1, hyperintense-isointense on T2 and significantly contrast enhanced.
NACC is a malignant epithelial tumor of the salivary glands, occurring most frequently in the 5th decade of life, without sex predilection. It is the most common malignancy of the submandibular and minor salivary glands.
In the nasopharynx, NACC can vary in presentation from an asymptomatic mass to severe ear and neurological symptoms, such as ear pain, fullness, tinnitus, hearing loss, facial pain, unilateral migraine-like headache, paresthesias, numbness, sensory loss across the trigeminal nerve course, abducens or oculomotor nerve deficits.
Dong J, Zhang L, Mo Y, Tian L, Liu L, Wu P. Discovery of Invasion Routes for Nasopharyngeal Adenoid Cystic Carcinoma. J Cancer 2015; 6(1):90-97. doi:10.7150/jca.10739. Available from https://www.jcancer.org/v06p0090.htm
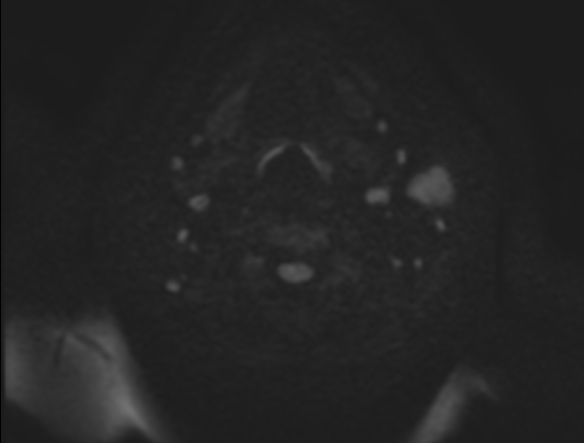
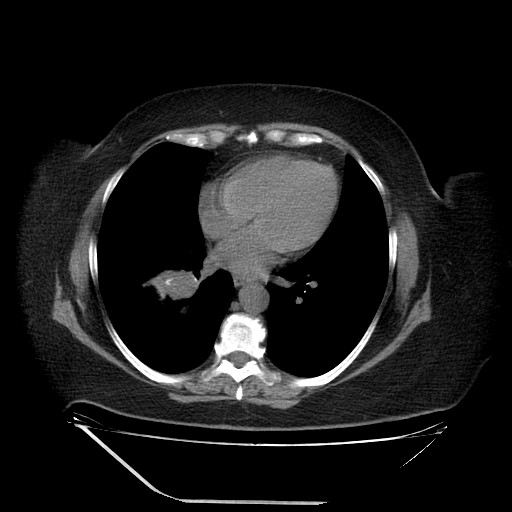
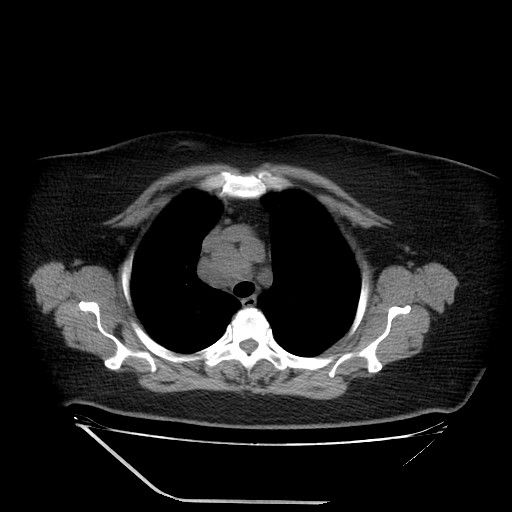
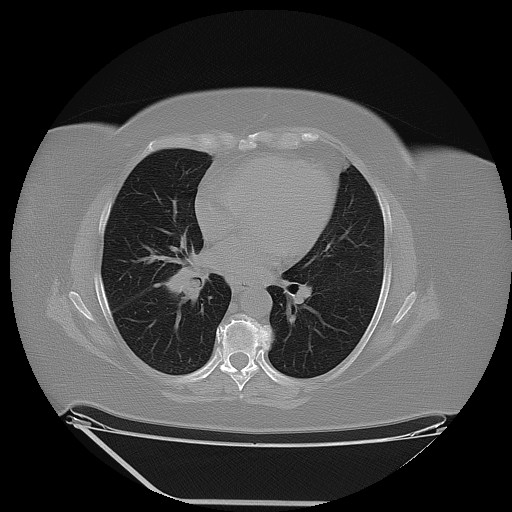
Parotid gland is an uncommon metastatic site for non-head and neck primary tumours. Metastatic tumours found in the parotid gland more commonly originate from primary head and neck cancers, while those originating from non-head and neck sites constitute 13% of metastatic lesions found in the parotid. Of the various non-head and neck primary tumours, lung cancer is the most common site of origin with other previously reported sites include renal, breast, colon and gynaecological carcinomas, as well as lymphomas.
It is postulated that these infraclavicular tumours usually affect the parotid parenchyma by means of haematogenous spread, while primary head and neck malignancies tend to spread to the parotid lymph nodes via the lymphatics.
MTS involving males with a median age of 60 years (range 40–74 years).
Although it is extremely rare, a potential metastasis of lung cancer should not be ignored in the diagnosis of a parotid tumor. Preoperative routine examinations such as a chest X-ray and lung CT, may play an important role in the differential diagnosis.
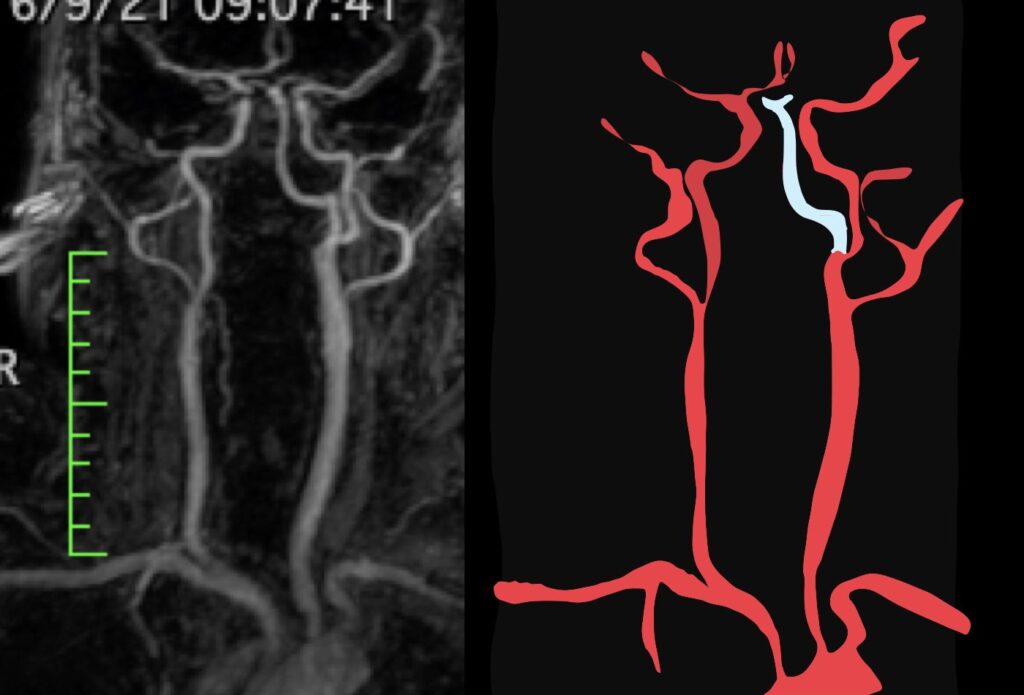
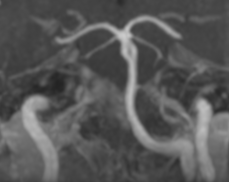
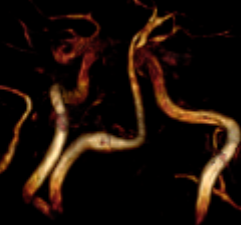
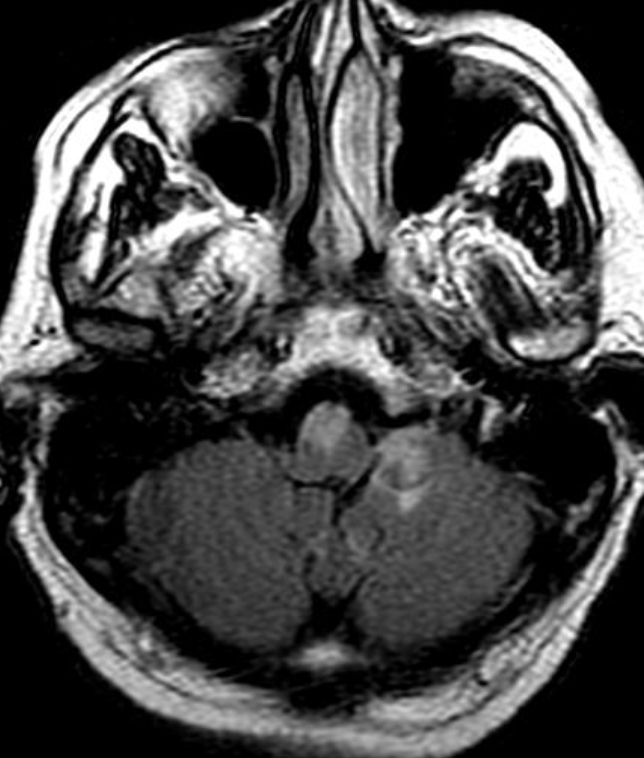
The persistent hypoglossal artery is the second most common carotid-basilar anastomosis. the prevalence is 0.1% to 0.2%. the primitive hypoglossal artery originates from the cervical part of the internal carotid artery at the level of C-1 to C-3.
After a tortuous course, it penetrates the enlarged hypoglossal canal and joins the lower portion of the basilar artery. When it is large, the proximal vertebral arteries usually are hypoplastic and the ipsilateral vertebral artery may be absent. the persistent hypoglossal artery is more frequent in females and on the left side as in our case.
The proatlantal intersegmental artery enters the posterior fossa through the foramen magnum, following the course of the vertebral artery. Therefore, differentiation between these primitive arteries on MR will be easy by demonstrating the foramen through which it passes.
This vascular anastomosis may be of functional importance in patients with carotid stenosis and may provide a pathway for cerebral embolism.
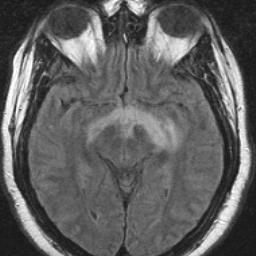
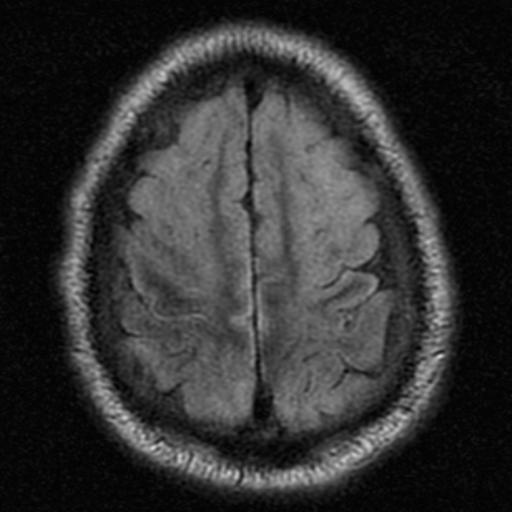
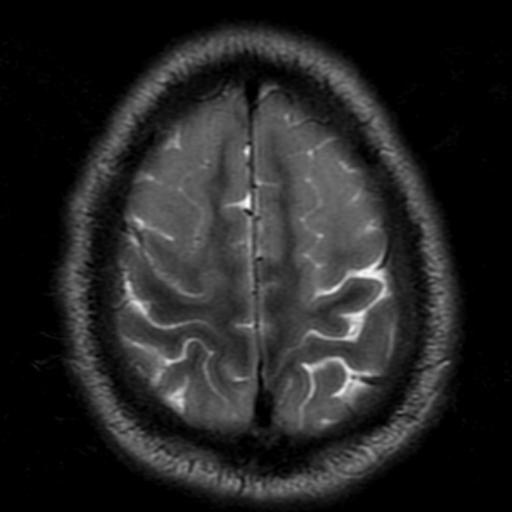
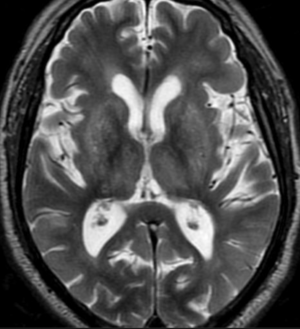
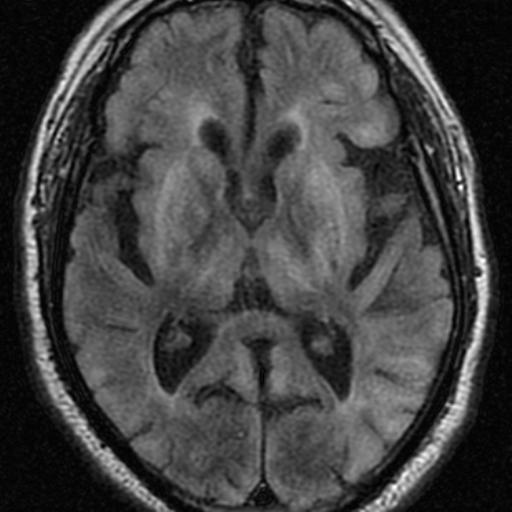
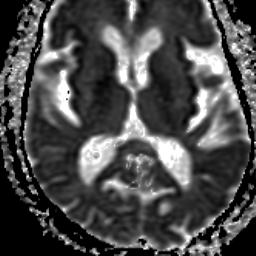
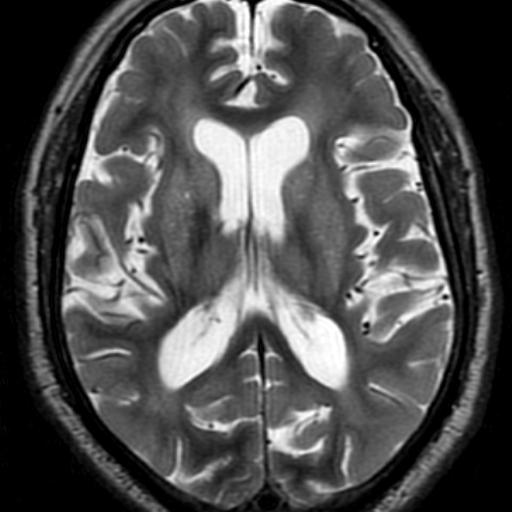
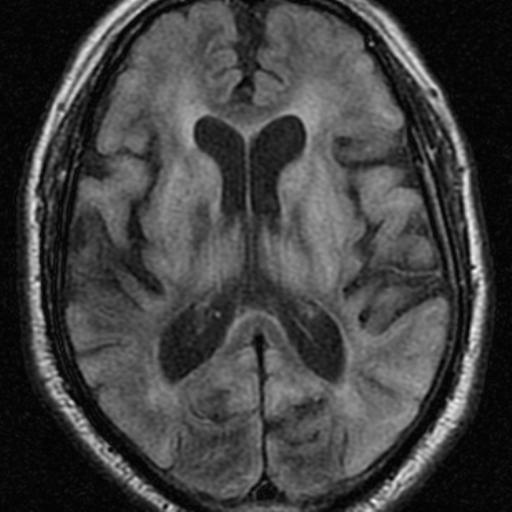
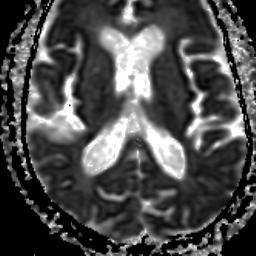
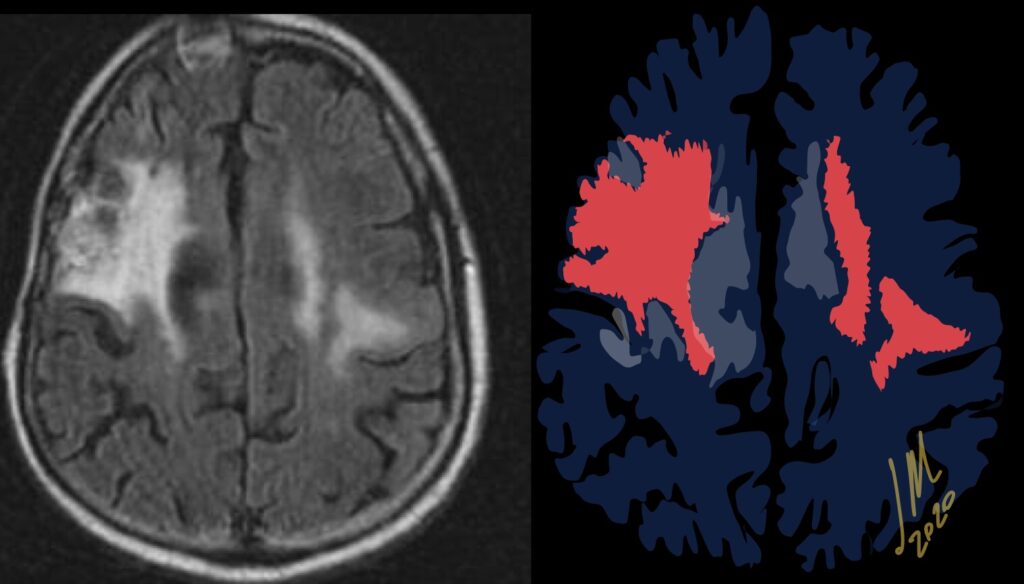
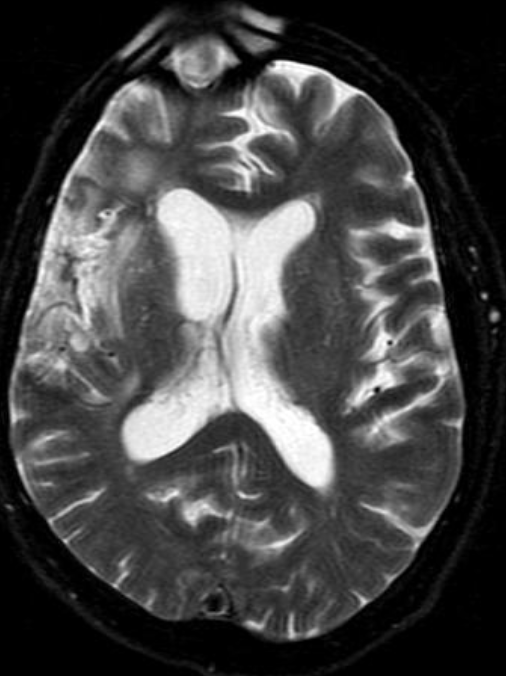
Hypoxic-ischemic encephalopathy (HIE) is the result of decreased global perfusion or oxygenation. The distribution of HIE varies according to the duration, degree, and abruptness of the hypoxic and/or ischemic insults, basal blood low, and metabolic activity in the areas of ischemia, temperature, and serum glucose levels. Layers 3, 4, and 5 of the cortex, watershed zones, and the hippocampi (cornu ammonis 1 zone) are sensitive to ischemia. DW hyperintensity throughout the cerebral cortex suggests devastating diffuse hypoxic-ischemic necrosis, whereas a pattern of basal ganglia or thalamus suggests primary hypoxic injury or mild HIE. Imaging Features include; Symmetric T2/FLAIR hyperintensity in deep gray nuclei and cortex.
The location of the injury correlates with the severity; mild to severe> Watershed zone infarcts, Gray matter, basal ganglia, sensorimotor and visual cortex, cerebellum( in older patients)and hippocampi.
Reference:
Diffusion-Weighted MR Imaging of the Brain Moritani . Ekholm . Westesson. P- 172
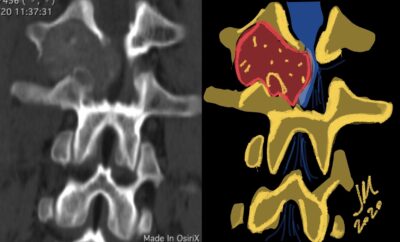
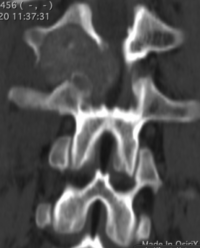
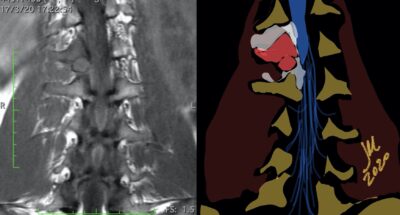
OBs are very rare and constitute about 1% of all primary bony tumors. These tumors tend to involve long bones and vertebral column. OBs are rare primary bony tumors constituting only 1% of all cases.
In 1984, a borderline osteoblastic tumor entity called “aggressive osteoblastoma” was introduced by Dorfman and Weiss and was found to be associated with a high recurrence rate and potential for malignant transformation. Despite being benign tumors, osteoblastomas often cause pronounced bone destruction, soft tissue infiltration, and epidural extension. They usually behave aggressively with extensive uncontrollable local recurrence, and even malignant transformation with metastatic disease has been reported
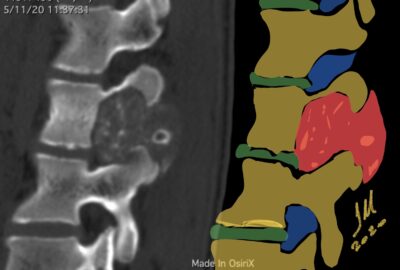
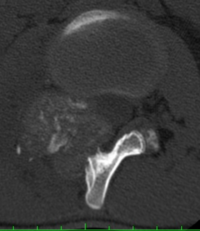
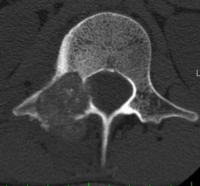
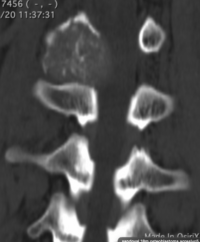
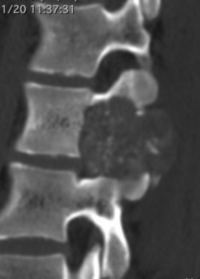
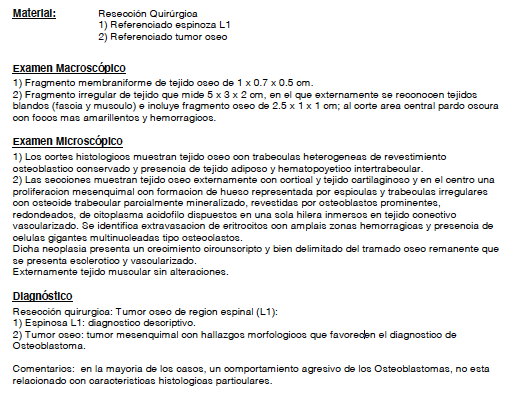
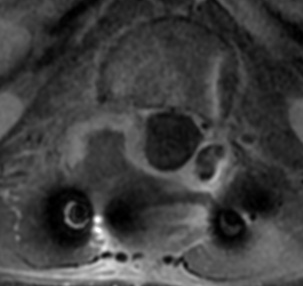
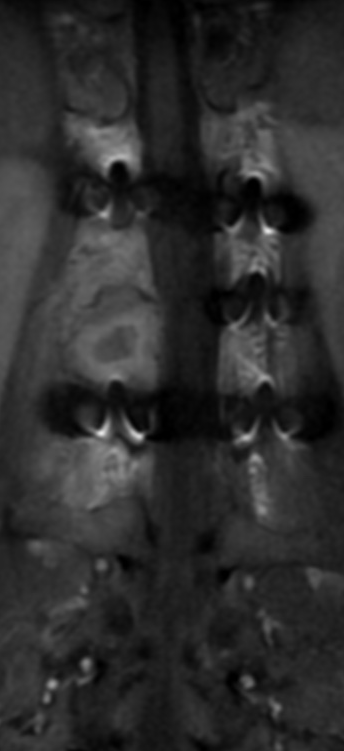
CT appearance of spinal osteoblastoma is a lytic expansile lesion with a shell of sclerosis, and soft tissue masses can be observed around the lesion.
The imaging features of spinal osteoblastoma on MRI are considered nonspecific. These lesions often display a low to isointense signal on T1-weighted MRI, whereas T2-weighted MRI demonstrates an intermediate- to high-intensity signal due to matrix calcification and intense enhancement representing the highly vascular nature of such lesions
Notably, however, this radiographic appearance may lead to overestimation of the limits of the tumor and can be somewhat confusing to orthopedic surgeons and radiologists, who may interpret these tumors as other clinical entities such as Ewing’s sarcoma or lymphoma
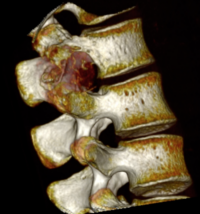
flare phenomenon
flare phenomenon” was described by Crim et al. in 1990. Specifically, these neoplasms often cause a diffuse, reactive prostaglandin (PG) – mediated inflammatory infiltrate within adjacent vertebrae surrounding paraspinal soft tissues. In contrast, for aggressive osteoblastoma in the spine, the tumor may be an expansile lesion with a multitude of small calcifications, a prominently clerotic rim, and paravertebral and epidural extensions and may also radiographically mimic aneurysmal bone cysts, osteosarcomas, or bone metastases.
flare phenomenon
Another essential diagnostic tool is bone scintigraphy, which is the most sensitive radiographic scan described in the literature for osteoblastoma and typically shows increased radiotracer uptake, indicating increased osseous turnover
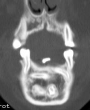
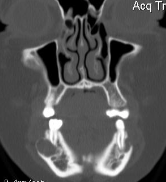
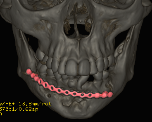
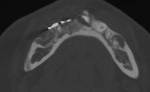
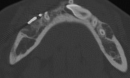
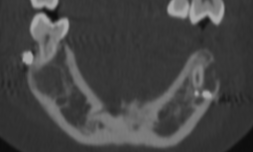
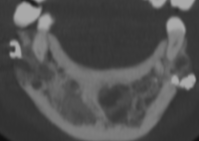
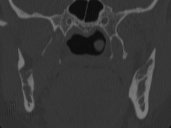
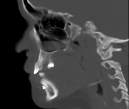
Cherubism is a rare osseous disorder of children and adolescents. Although the radiologic characteristics of cherubism are not pathognomonic, the diagnosis is strongly suggested by bilateral relatively symmetric jaw involvement that is limited to the maxilla and mandible. Imaging typically shows expansile remodeling of the involved bones, thinning of the cortexes, and multilocular radiolucencies with a coarse trabecular pattern.
Cherubism has been described as a subtype of fibrous dysplasia, specifically a hereditary craniofacial fibrous dysplasia, because of the radiographic similarities between the conditions. Recent genetic analysis, however, has shown them to be separate entities. The genetic basis for cherubism was identified in 1999, when the gene responsible for it was mapped to chromosome 4p16.3.
16F. 1 TC
Although the radiologic and histologic characteristics of cherubism are not pathognomonic, the overall morphologic features are characteristic and consistent among cases; these features therefore allow an accurate prospective diagnosis in the appropriate clinical setting.
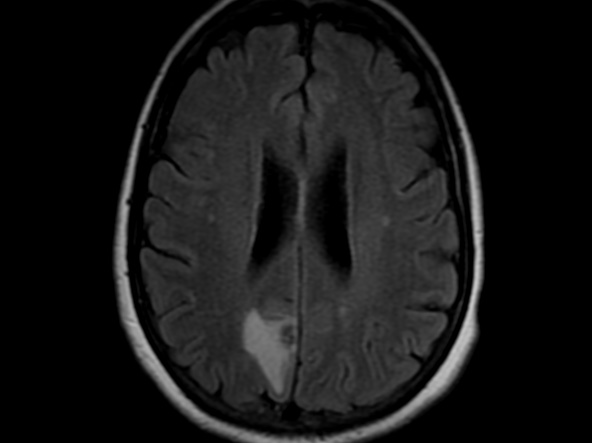
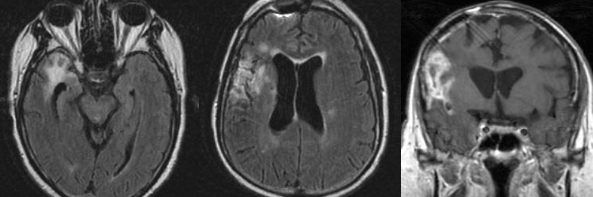
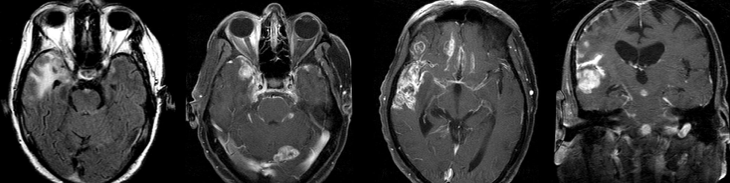
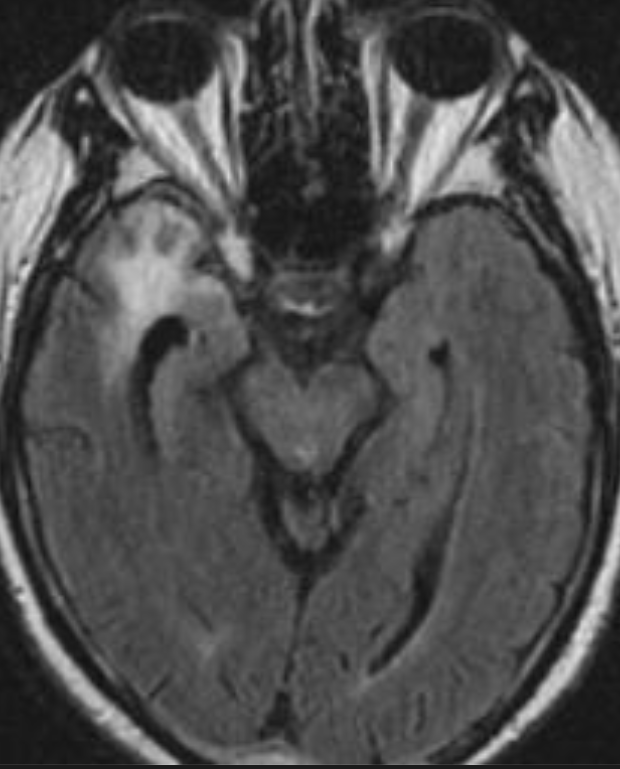
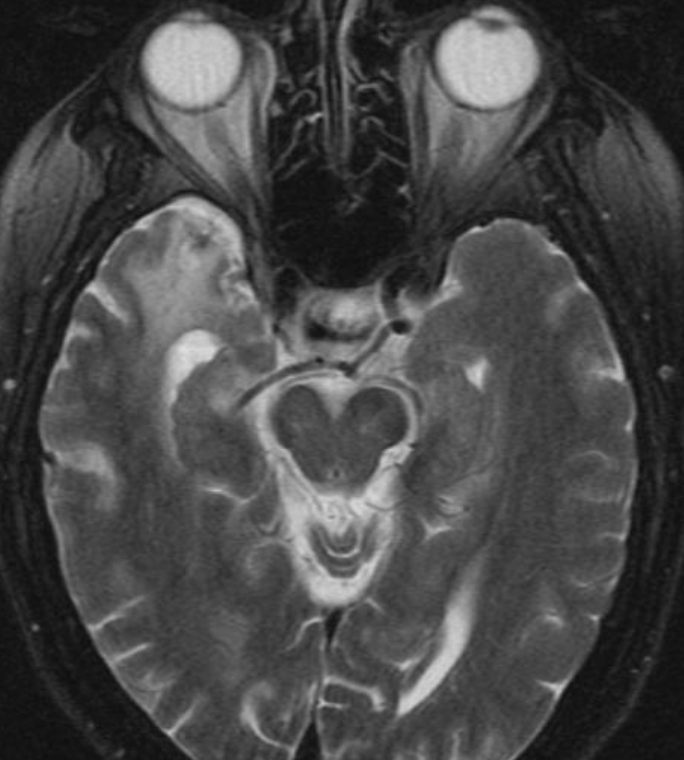
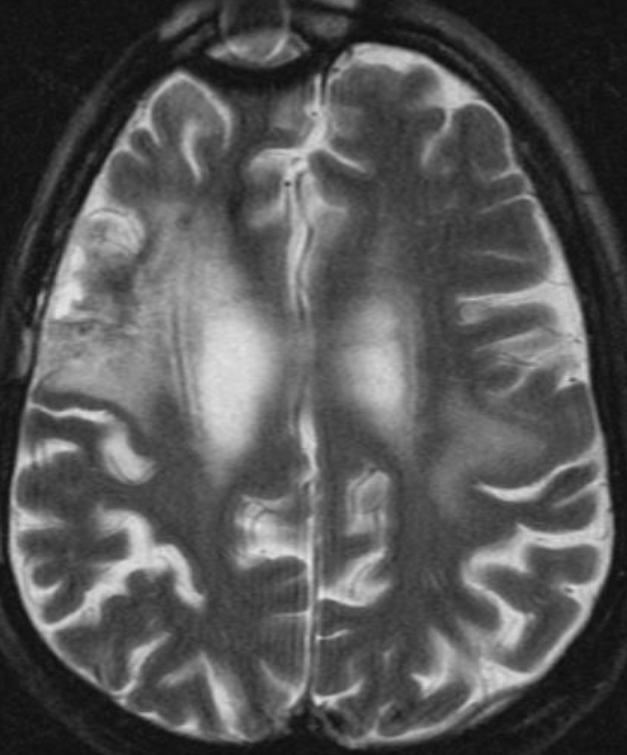
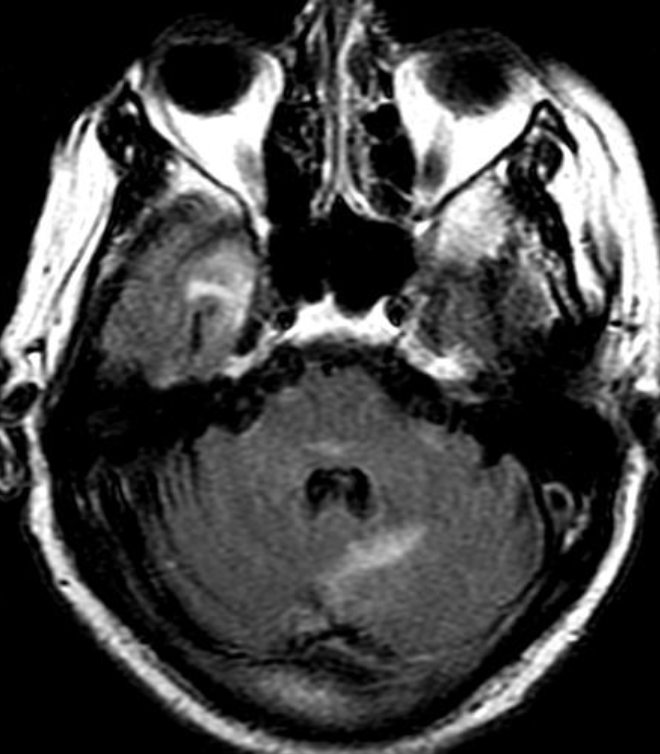
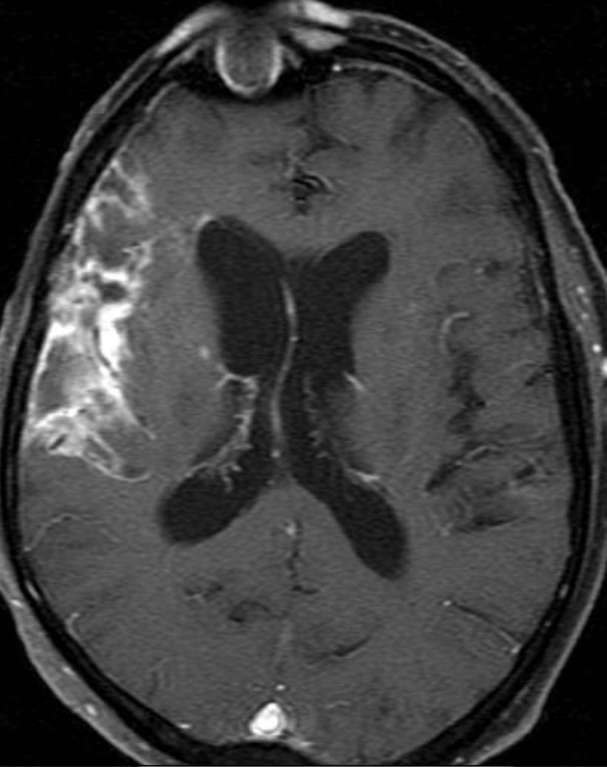
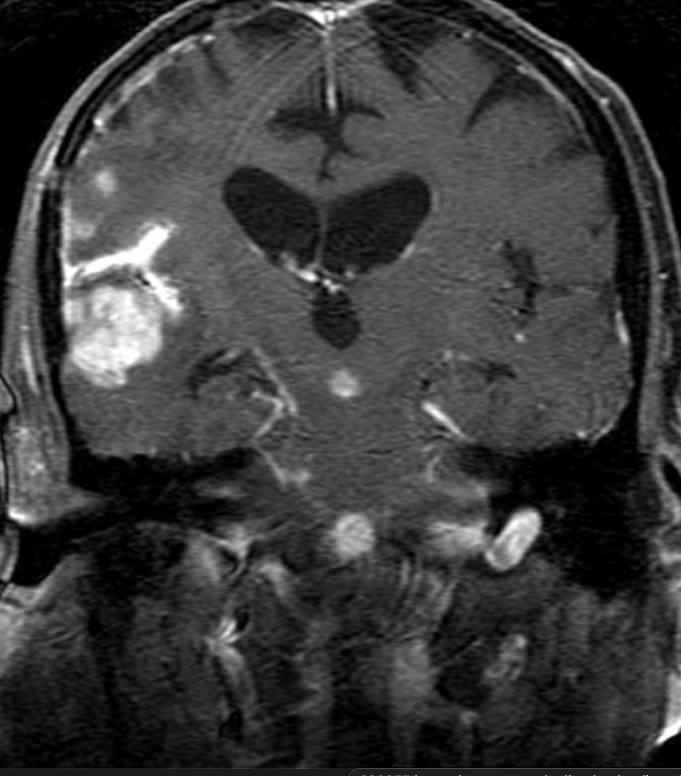
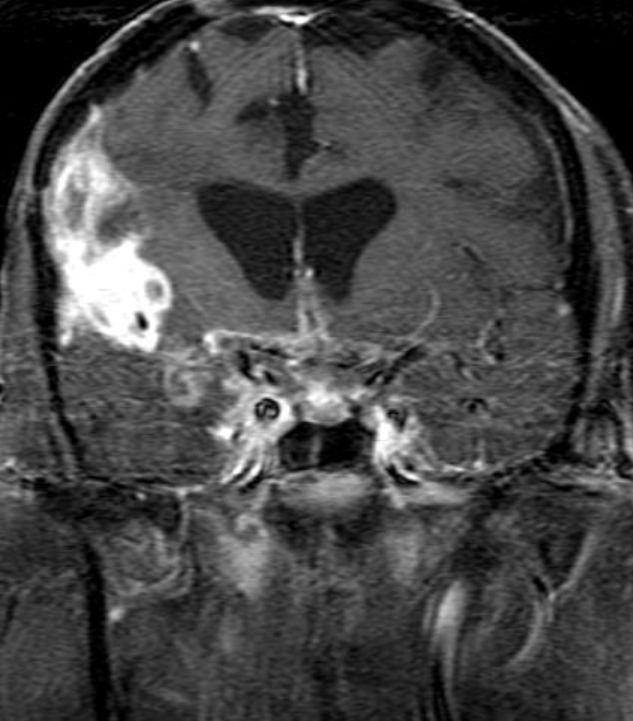
Cerebral radiation necrosis is a serious late delayed complication that manifests after a latency period of several months, although the range is broad and cases have been reported more than 10 years after irradiation. Histopathologic features of radiation necrosis include fibrinoid changes in the blood vessels, coagulative necrosis, demyelination, and gliosis. The disruption of the BBB (as visualized on gadolinium-enhanced images) may be mediated in part through vascular endothelial growth factor (VEGF) that is released in response to hypoxia. The reported incidence of radiation necrosis after RT for brain tumors ranges from 3% to 24%. Radiation necrosis is more likely to occur when high doses per fraction are administered, and combined use of chemotherapy with RT may play a role in development of treatment-related necrosis. Targeted therapy and immunotherapy may also increase the risk of treatment-related necrosis. Radiation necrosis typically develops at or adjacent to the original site of the tumor, the location that received the highest radiation dose. Radiation necrosis can also develop in part of the normal brain parenchyma that was included in the treatment field of a tumor outside the brain. In many cases, radiation necrosis is a self-limiting process that can be managed conservatively without intervention, although some patients need steroids for symptomatic relief.
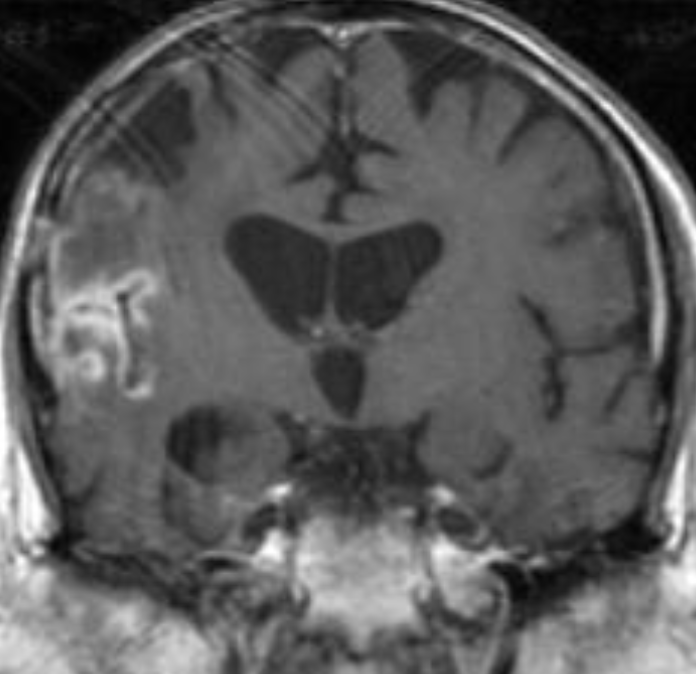
Conventional MRI typically demonstrates an enhancing mass lesion with central necrosis and reactive edema. The enhancement pattern is often described as “spreading wavefront,” meaning that the margins of the enhancement are ill defined or “soap bubble–like” or “Swiss cheese–like,” meaning that the enhancing lesion includes central nonenhancing necrotic components of varying size. Multiple lesions are possible, and some lesions may develop distant from the original site of the tumor if the distant site was in the radiation field
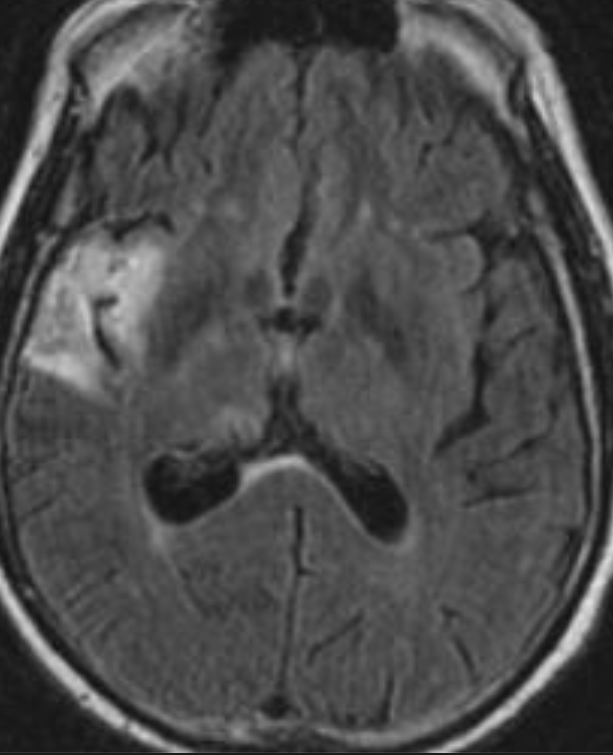
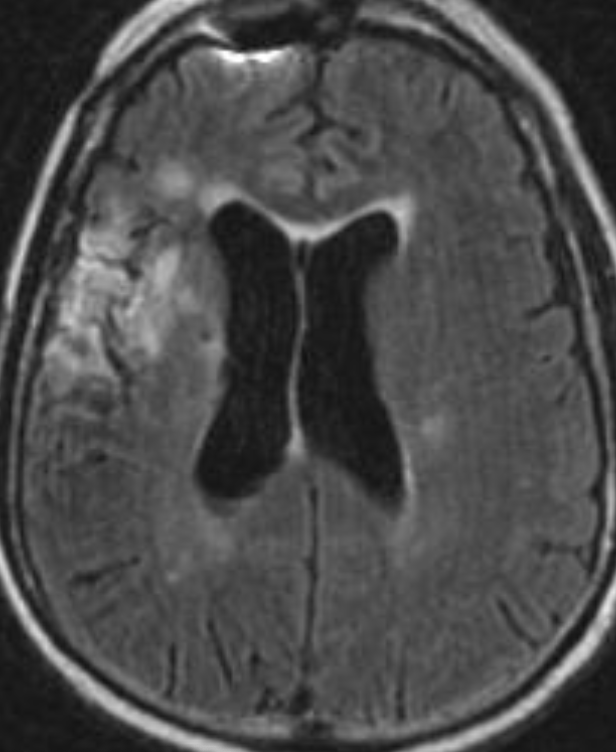
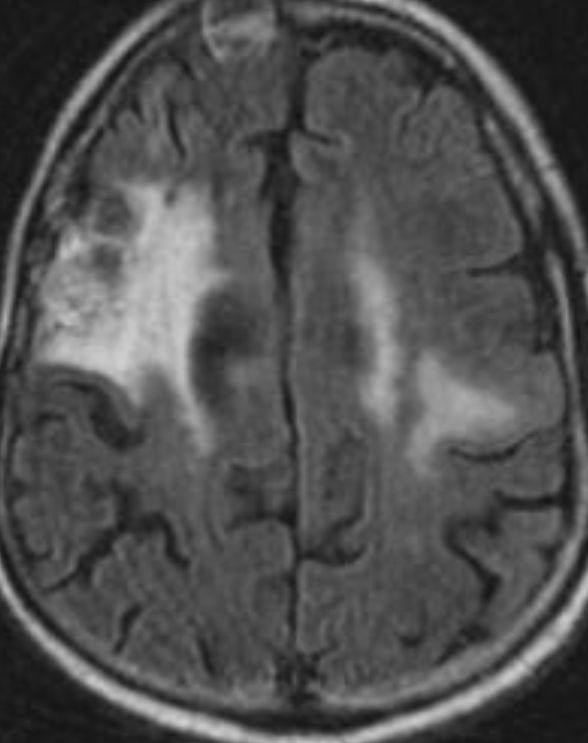
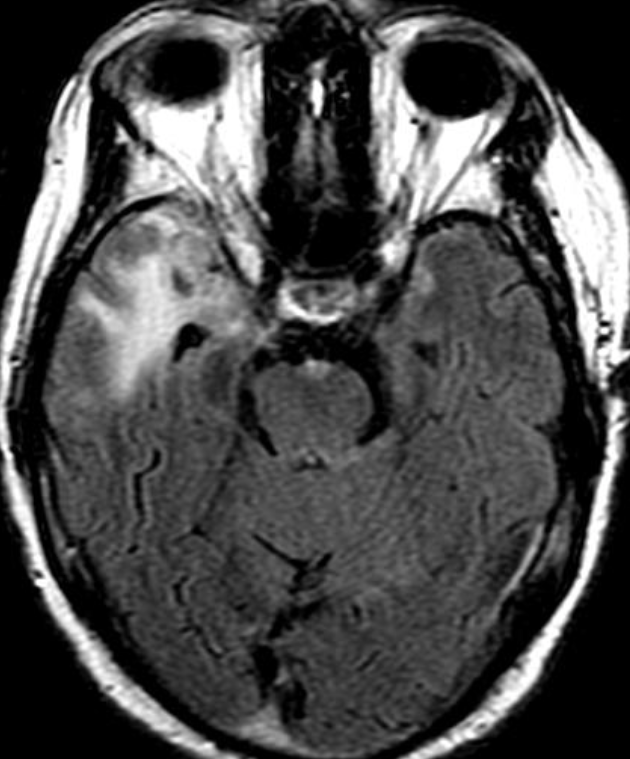
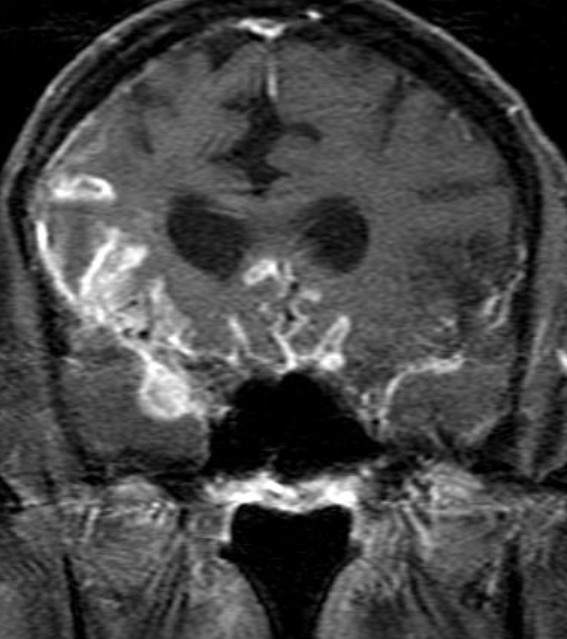
Radiation necrosis.
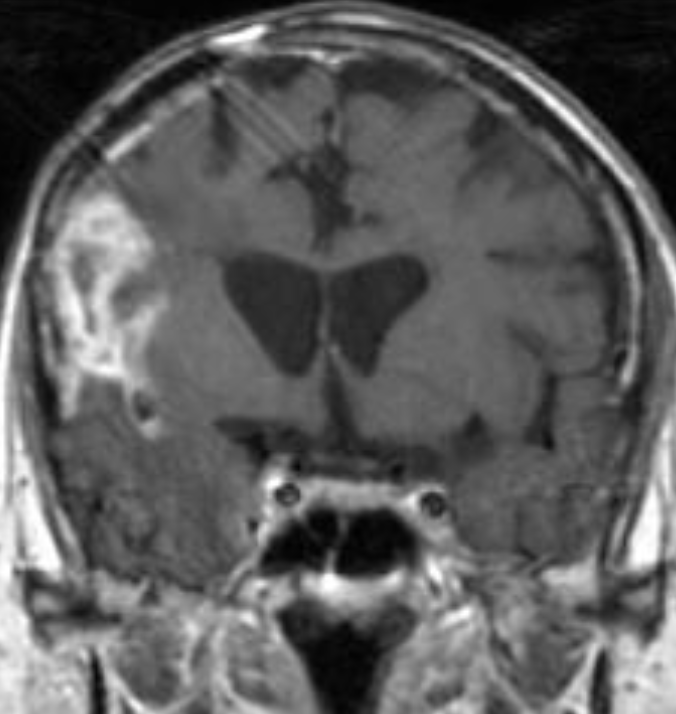
As radiation necrosis progresses with tumorlike growth, it can lead to marked shrinkage of the white matter and cortex and result in focal brain atrophy. The periventricular white matter is among the areas most susceptible to radiation necrosis. This may be explained by this neuroanatomic region having relatively poor blood supply from long medullary arteries that lack collateral vessels, making it vulnerable to ischemic effects produced by postirradiation vasculopathy. Imaging findings of radiation necrosis are not always irreversible and progressive but can be static, decrease, or even resolve at follow-up . White matter lesions were the earliest and most common manifestation after RT, followed by enhancing lesions, which often became necrotic with increasing size. Both white matter lesions and enhancing lesions were more likely than cysts to regress, and both could show complete resolution. Cysts were the least frequent pattern of radiation-induced injury and developed from enhancing lesions that exhibited necrosis
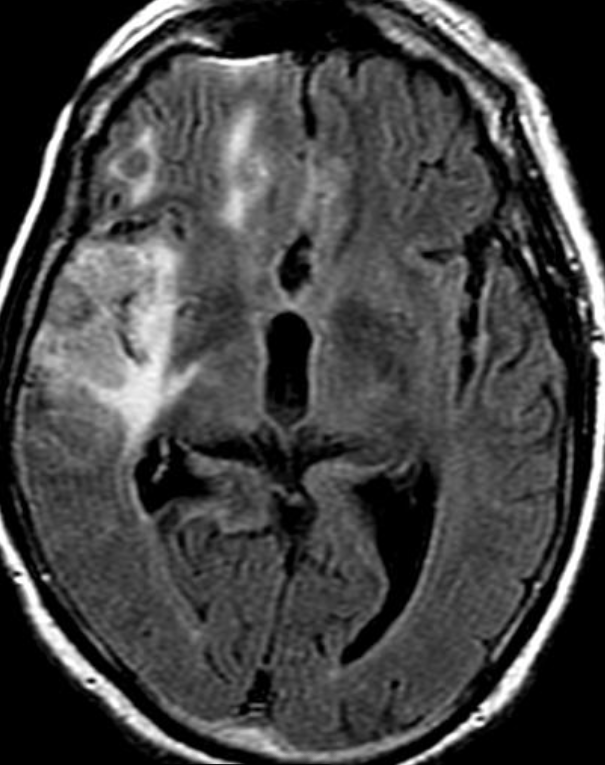
Conventional Imaging for Distinguishing Radiation Necrosis from Tumor Recurrence
Radiologic features of radiation necrosis at conventional imaging overlap with those of recurrent tumors, including high-grade primary brain tumors and brain metastases; therefore, image interpretation can be challenging. Biopsy of the suspicious lesion may be required for a definitive diagnosis, particularly in patients who are symptomatic and have worsening imaging findings over time. However, it is known that even at histopathologic analysis, residual or recurrent tumor mixed with radiation necrosis is a common finding.
Although not always reliable, some clinical or imaging features have been suggested in previous reports and may aid in diagnosis of radiation necrosis and tumor recurrence. First is the time elapsed since RT. Radiation necrosis usually manifests after a latency period of many months (12 months average) a new or worsening abnormality starting 3 years after RT is unlikely to be due to pure radiation necrosis. Corpus callosum involvement in conjunction with multiple enhanced lesions—with or without crossing of the midline and subependymal spread—were statistically significant, favoring predominant glioma recurrence
MR spectroscopy attempts to identify tumor recurrence by providing information on metabolic changes. Recurrent brain tumors exhibit high ratios of choline/creatine (Cho/Cr) and choline/N-acetylaspartate (Cho/NAA) whereas radiation necrosis exhibits increased lactate and lipid peaks .
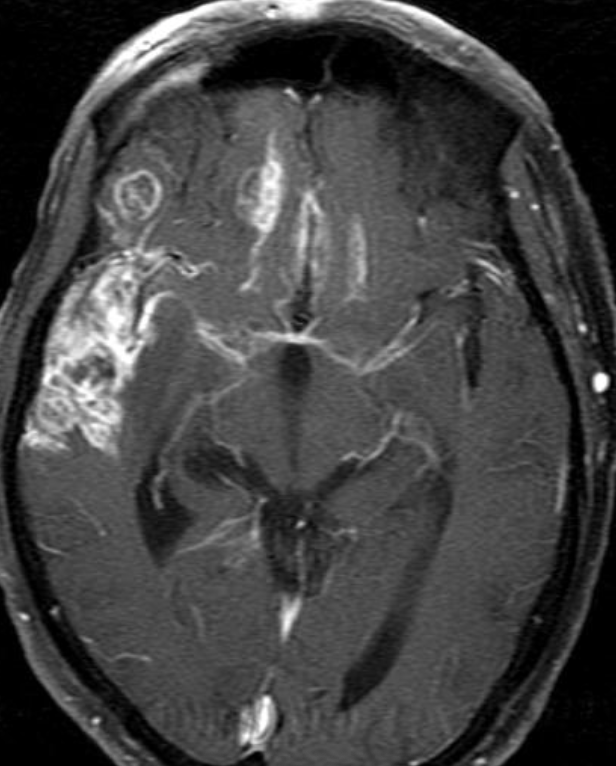
Dynamic susceptibility contrast (DSC) MRI is the most widely used perfusion technique for brain tumors. DSC perfusion MRI relies on the T2- and T2*-shortening effects of gadolinium-based contrast agents and involves rapid imaging to capture the signal intensity changes due to the first passage of an intravenously administered contrast agent bolus.
The main parameter derived from DSC MRI in the context of brain tumors is relative cerebral blood volume (rCBV). rCBV is an indirect index of cerebral blood volume, generally calculated relative to region of interest (ROI) values in the contralateral normal white matter. Radiation necrosis typically causes hypoperfusion with reduced rCBV, whereas high-grade tumor recurrence results in high rCBV.
Oligo RT
The only method of distinguishing pseudoprogression and true tumor progression is to perform follow-up examinations of the patient because conventional MRI does not allow differentiation of the two conditions. Imaging may be regularly performed at 2–3-month intervals throughout the follow-up period although the frequency of imaging can be variable across institutions. In clinical practice, the following features can be helpful: (a) presence of symptoms and (b) methylation status of the MGMT gene promoter.
Recurrence
In the central nervous system, the effects of radiation can be roughly divided into effects on vascular endothelial cells and direct effects on neuroglial cells, in particular the oligodendroglial cells.
Vascular endothelial damage causes altered permeability, leading to vasogenic edema and disruption of the blood-brain barrier (BBB) or blood–spinal cord barrier. Preclinical studies suggest that endothelial damage may occur within the first 24 hours after irradiation. Endothelial damage can lead to other late vascular effects, such as telangiectasia, thrombosis, occlusion of small vessels, fibrinoid deposits, and hyaline thickening of vessel walls. As a result, ischemic stroke or hemorrhage may occur months to years after RT.
Oligodendrocytes are the most radiosensitive type of glial cell, with cell death occurring rather early after relatively low doses of irradiation. Radiation not only reduces the number of mature oligodendrocytes but also induces loss of their precursors, the oligodendrocyte type 2 astrocyte. This results in failure to replace normally turned over oligodendrocytes, with the eventual consequence being demyelination. In addition, there are changes in cellular composition such as increased numbers of reactive astrocytes (gliosis) and microglia. These reactive cells have been reported to produce reactive oxygen species, proinflammatory cytokines, and growth factors (eg, vascular endothelial growth factor [VEGF]), leading to a cycle of further cellular toxic effects and tissue damage .
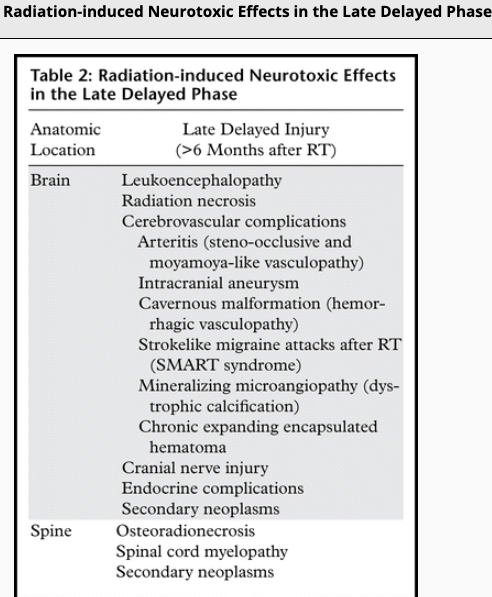
Radiation-induced injury can be divided into three phases: acute, early delayed and late delayed. Acute and early delayed injuries are usually transient and reversible, whereas late delayed injuries are generally irreversible. Keys to recognizing radiation-induced changes at follow-up imaging are knowledge of (a) the amount of time elapsed since RT, (b) the location of the target lesion, and (c) the amount of normal structures included.