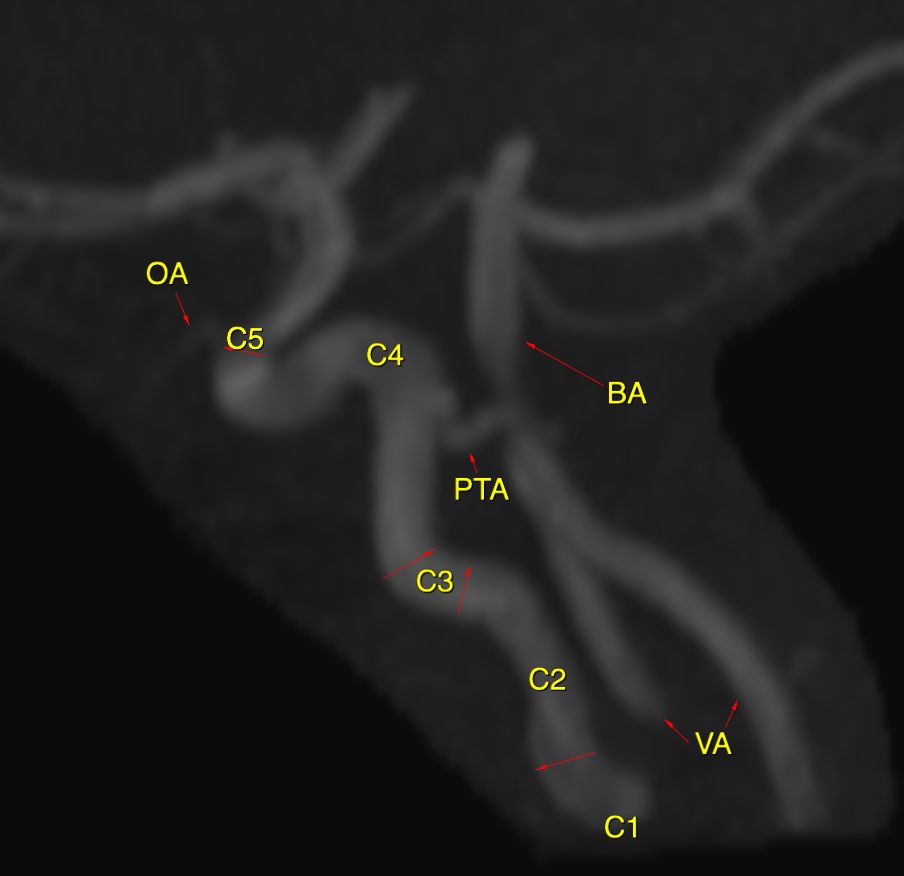
Saltzman first described the angiographic appearance of PTA and its classification into three types according to angiographic appearance.
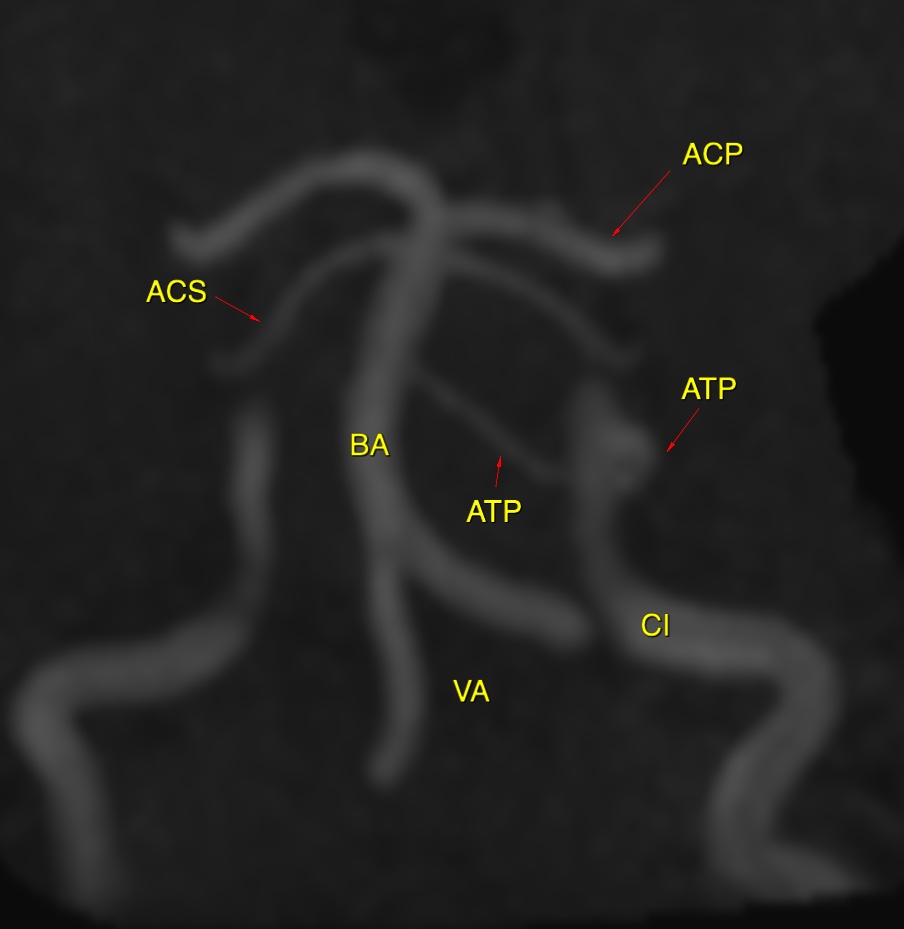
The Saltzman type I PTA connects the basilar artery at the level between superior cerebellar artery (SCA) and AICA. The proximal basilar artery and posterior communicating artery are usually hypoplastic and subsequently both posterior cerebral arteries and SCAs are supplied through the PTA.
The Saltzman type II PTA connects the basilar artery above the origin of the SCAs. The posterior communicating arteries are present and provide the posterior cerebral arteries.
The Saltzman type III PTA is considered a combination of types I and II. Ali et al. reviewed Saltzman classification and included variations of PTA in type III, in which there is no connection of the basilar artery. The variations of PTA type III arise from the internal carotid and terminate directly as the SCA (type IIIa), AICA (type IIIb), and PICA (type IIIc) without interposition of the basilar artery.
In one study of 4.650 patients that underwent brain MRA, the prevalence of each type using the Saltzman classification was as follows: type I, 24%; type II, 16%; type III, 60%
Many authors state in their discussion that persistent trigeminal, hypoglossal, and proatlantal arteries have been associated with aneurysms distant from the persistent vessels. Such an association is dubious. The prevalence of aneurysms associated with persistent trigeminal artery is approximately 3%, which is similar to the prevalence of aneurysms in the general population.
Reference:
Chen YC, Li MH, Chen SW, Hu DJ, Qiao RH. Incidental findings of persistent primitive trigeminal artery on 3-dimensional time-of-flight magnetic resonance angiography at 3.0 T: an analysis of 25 cases. J Neuroimaging. 2011;21(2):152–8.
Cloft HJ, Razack N, Kallmes DF. Prevalence of cerebral aneurysms in patients with persistent primitive trigeminal artery.J Neurorsurg 1999;90:865–867
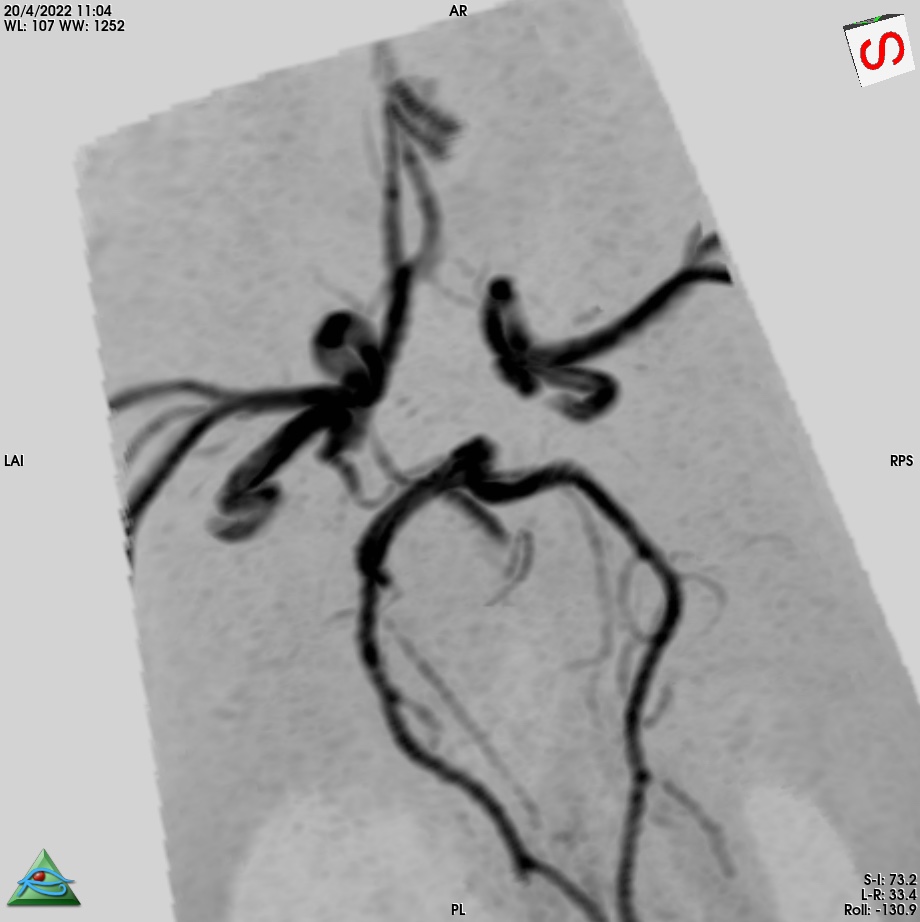
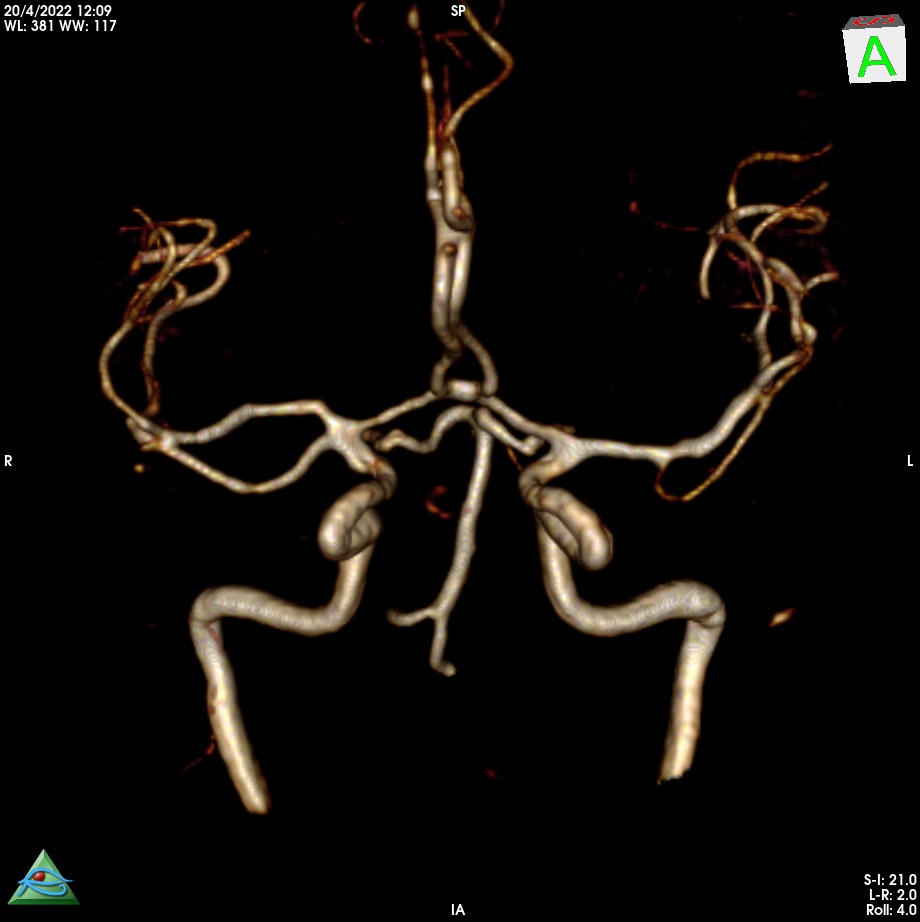
A duplicated middle cerebral artery (DMCA) is an anomalous vessel arising from the internal carotid artery (ICA). The origin of the DMCA lies between the anterior choroidal artery and the distal end of the ICA. Although there are several explanations of DMCA, its embryological origin is still an open question. Komiyama et al. proposed that the development of DMCA involves the anomalously early ramification of the early branches of the middle cerebral artery (MCA), based on their similarity to the cortical supply by the early branches of the MCA. Yamamoto et al. suggested that DMCA is a variant of the normal branching of the MCA. Kai et al. reported two types of DMCA : one with a course parallel to that of the main MCA (type A) and the other coursing toward the temporal lobe (type B).
DMCAs themselves have no clinical significance. However, rare aneurysms have been reported at the origin of the DMCA. It is unclear whether this association is a chance occurrence or is related by an unknown mechanism. Kai et al. reported that all aneurysms associated with DMCAs were found at the origins of type B DMCAs. They insisted that type B DMCAs can be expected to be subject to higher hemodynamic stress and that this is a factor in the development of aneurysms on the type B DMCA.
Reference:
Kai Y, Hamada J, Morioka M, Yano S, Kudo M, Kuratsu J. Treatment of unruptured duplicated middle cerebral artery aneurysm : case report. Surg Neurol. 2006;65:190–193. discussion 193
Asymptomatic patients with an elongated cord and a thick filum
Diagnosis and treatment of ATCS are a challenging task because of its rarity, and its presentation mimics a wide spectrum of pathologies. The clinical features of ATCS are widely recognized as nonspecific, including diffuse and nondermatomal back and leg pain. Other common symptoms include bladder dysfunction, skin abnormalities, scoliosis, and decreased motor and sensory function.
Tethered cord syndrome is a stretch-induced functional disorder of the spinal cord with its caudal part anchored by an inelastic structure. Garceau first described the “filum terminale syndrome” in 1953 in 3 patients. Yamada and others broadened the stretch-induced functional disorder to patients with other anomalies in 1981. Myelomeningocele, lipoma, lipomyelomeningocele, diastematomyelia, meningocele manqué, and dermoid sinus were included in this category but only when parallelism between the oxidative metabolic changes and neurologic status exists.
Symptoms related to a congenital tethered cord occur most commonly in childhood, so it was initially regarded as a pediatric problem; but in many patients, the diagnosis is not established until symptoms manifest in adulthood.
The second group includes asymptomatic patients with an elongated cord and a thick filum.
Three categories of TCS were recently described by Yamada and colleagues;
The first category includes lumbosacral cord anchored by an inelastic filum.
The second category includes caudal myelomeningoceles and many sacral myelomeningoceles.
The third category is divided into 2 groups. The first group includes patients with paraplegia and lipomyelomeningocele and myelomeningocele who apparently have no functional lumbosacral neurons. No neurologic benefit is expected from surgery in this group. The second group includes The second group includes asymptomatic patients with an elongated cord and a thick filum.
The incidence of occult spinal dysraphism is unknown, and although it is likely that some patients remain asymptomatic and a diagnosis is never made, a subset of patients with the congenital syndrome develops progressive symptoms and signs in adulthood.
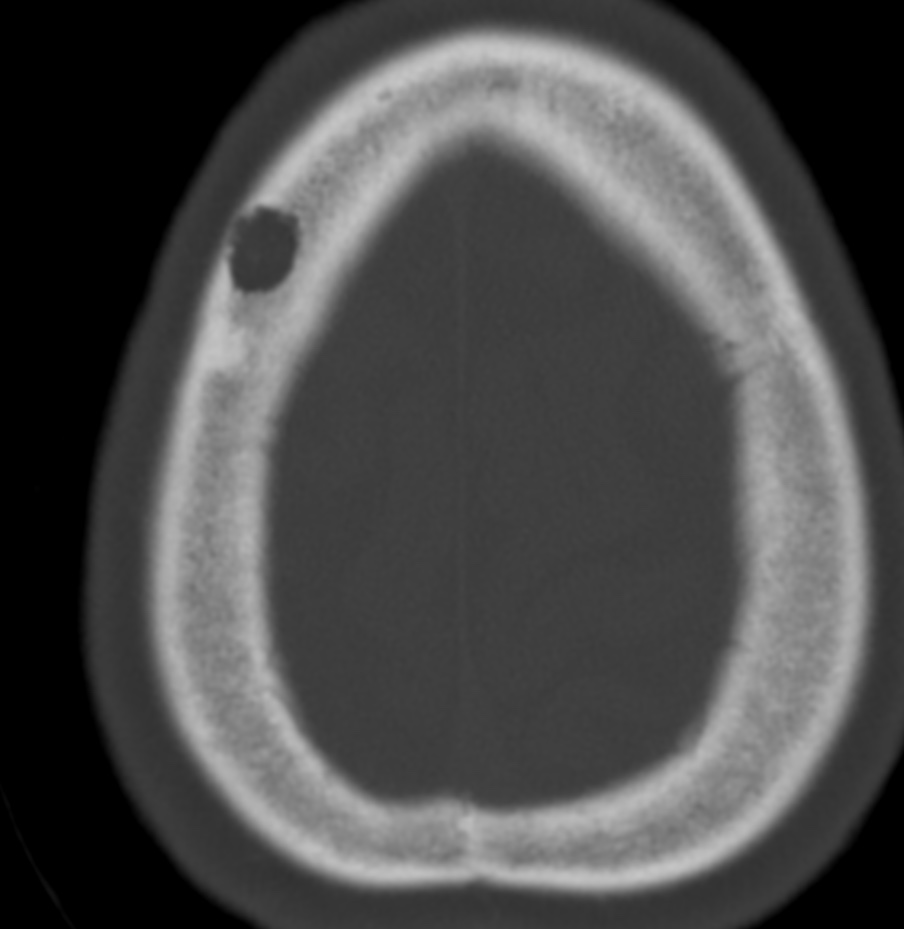
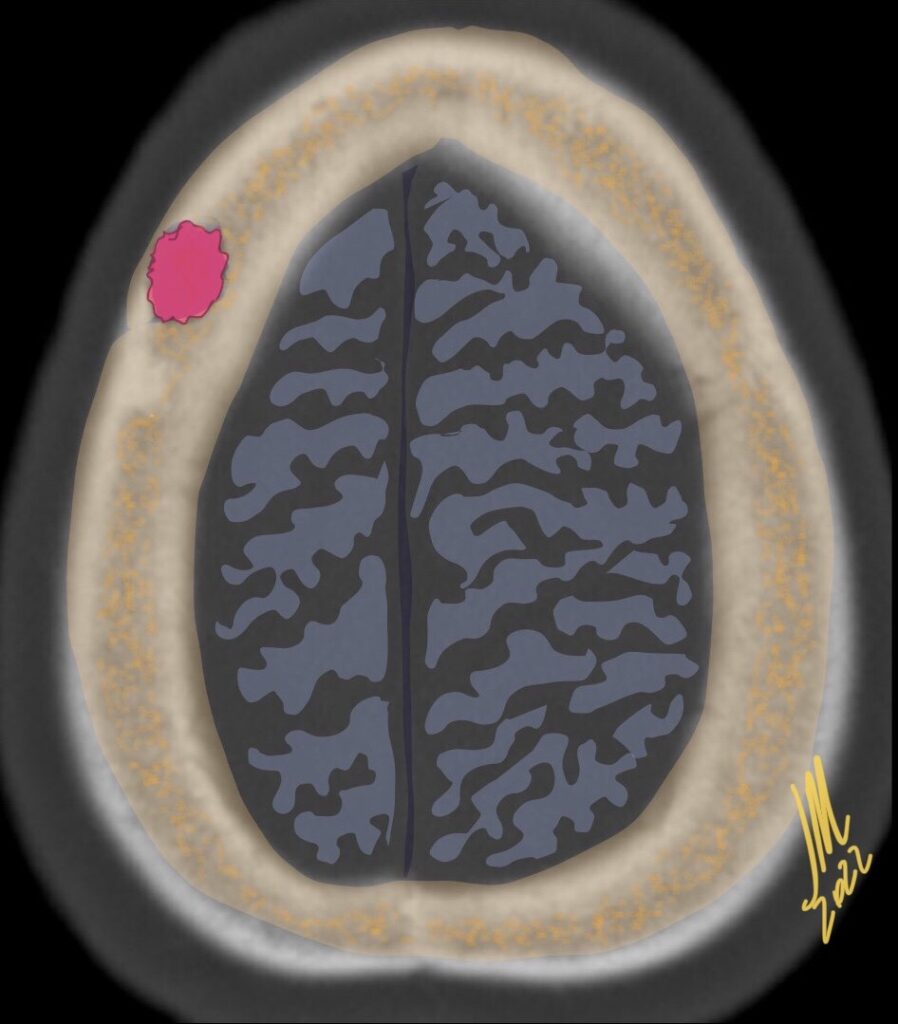
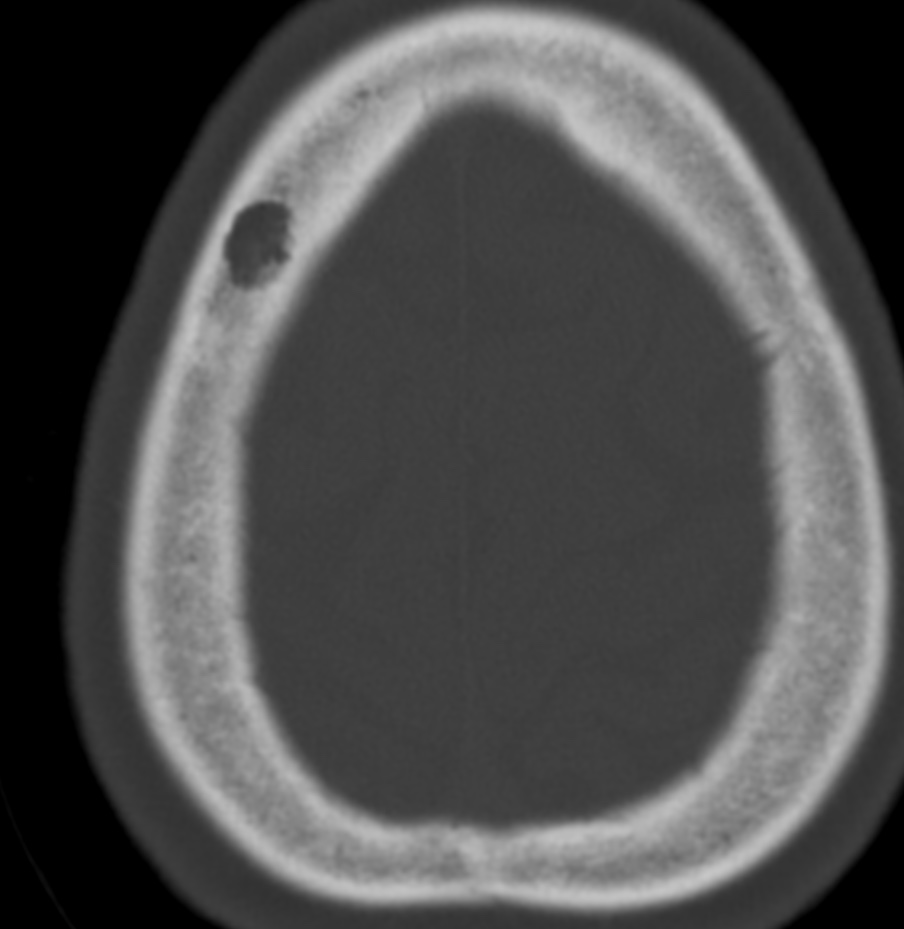
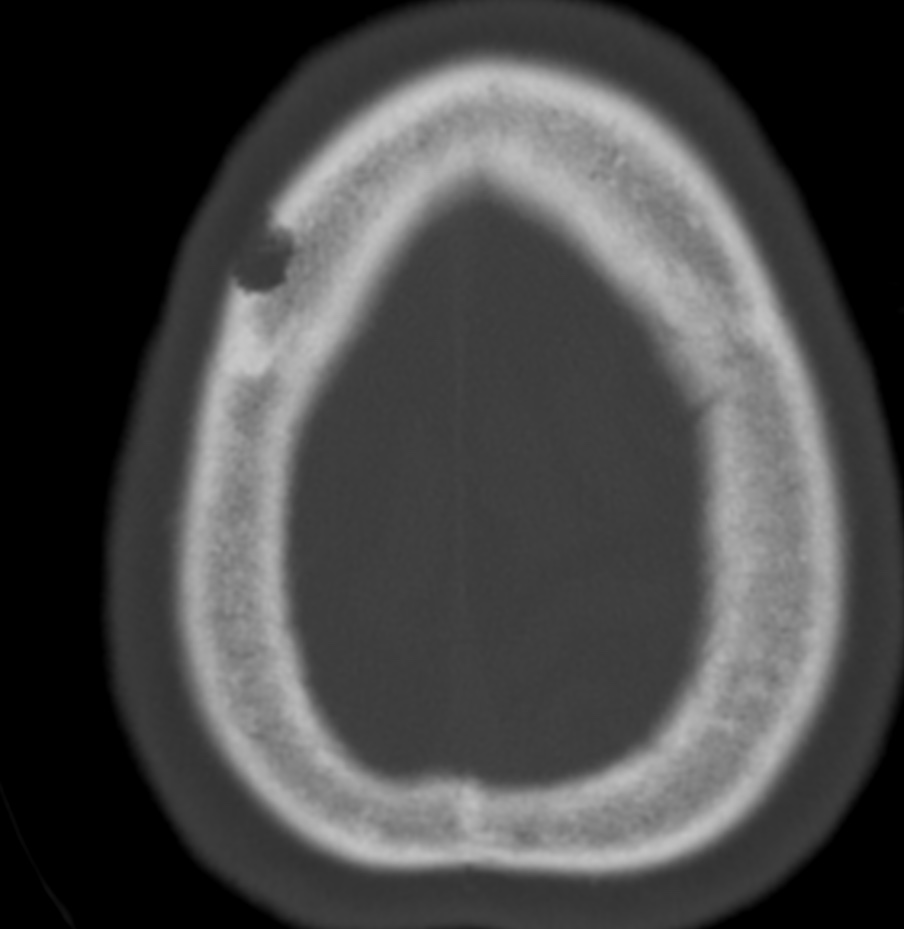
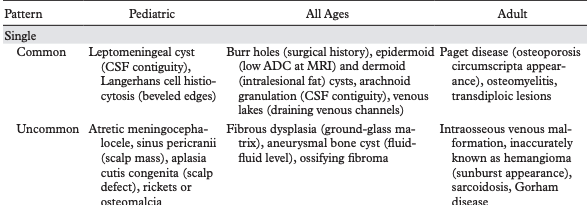
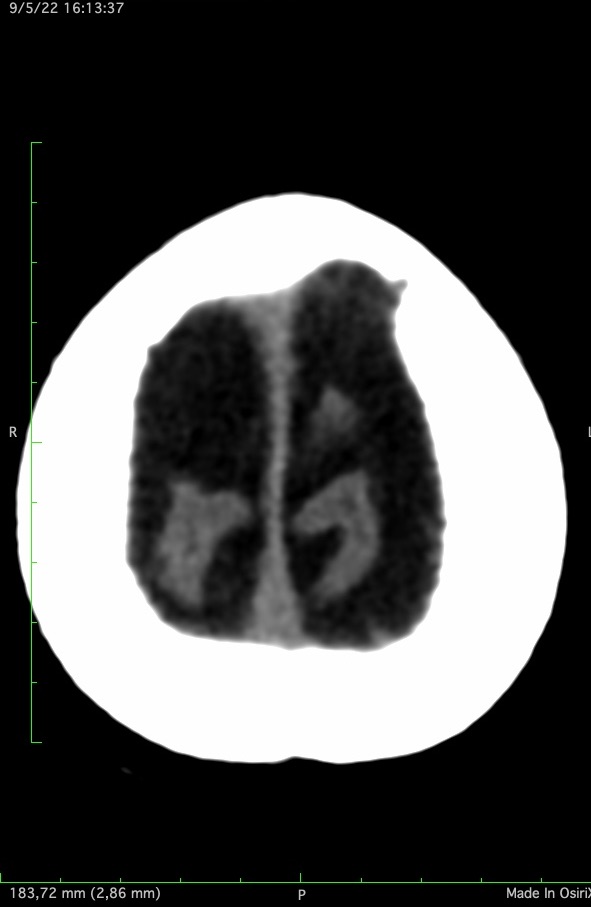
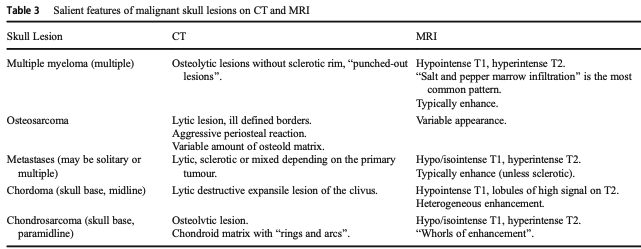
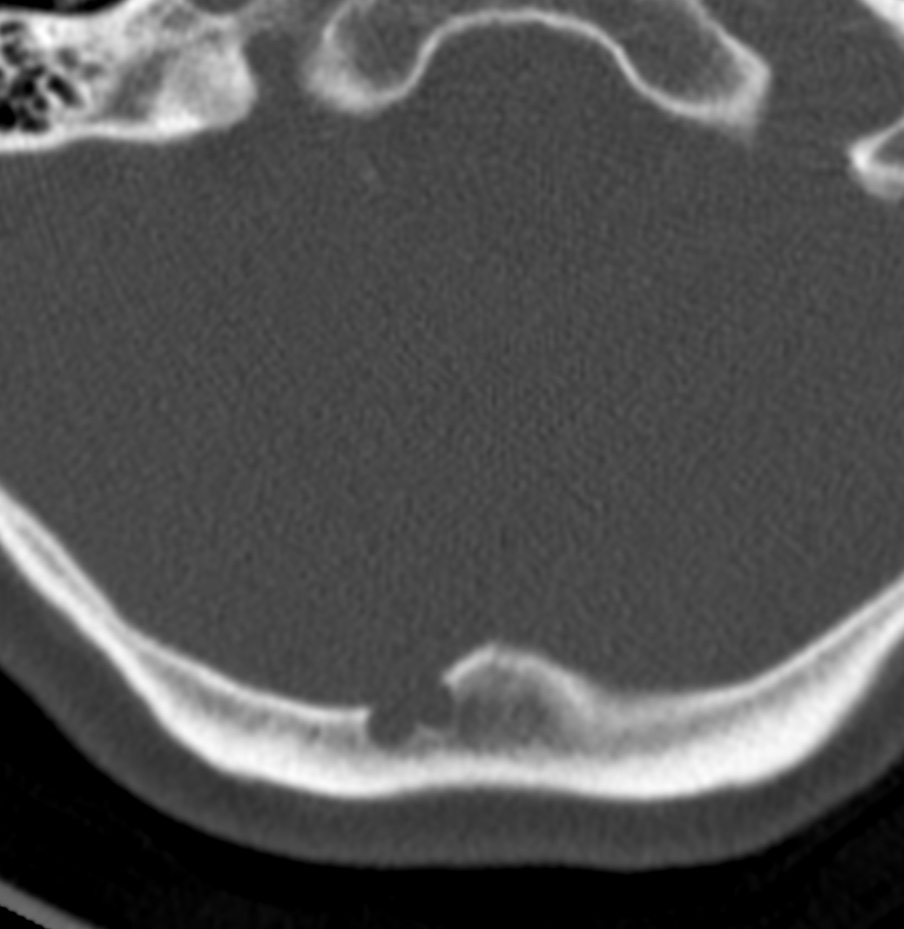
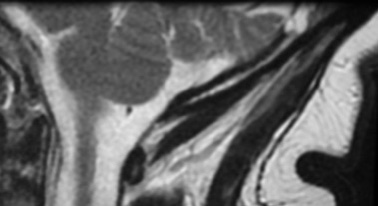
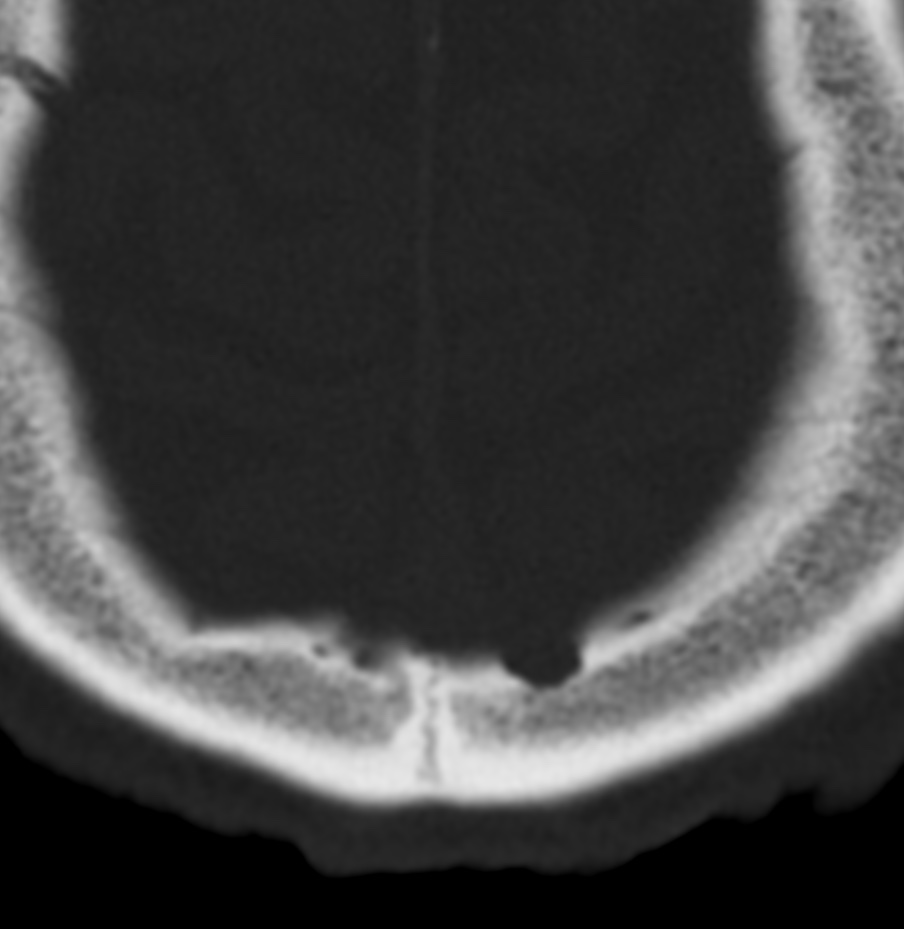
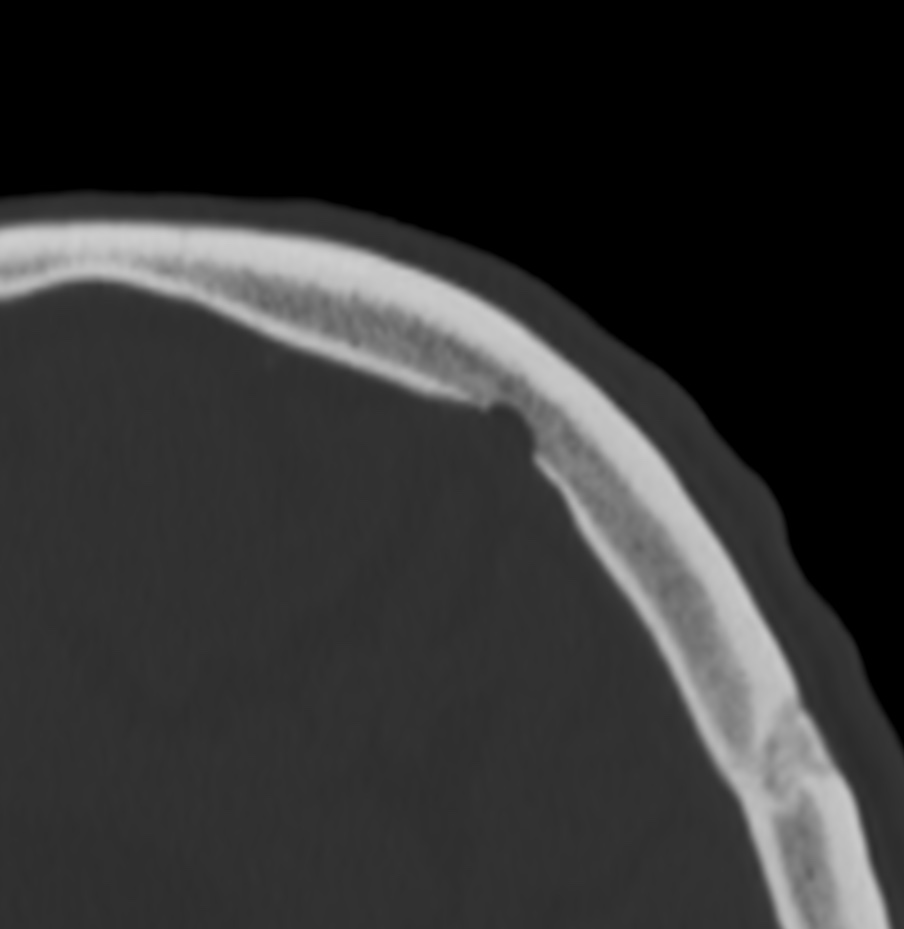
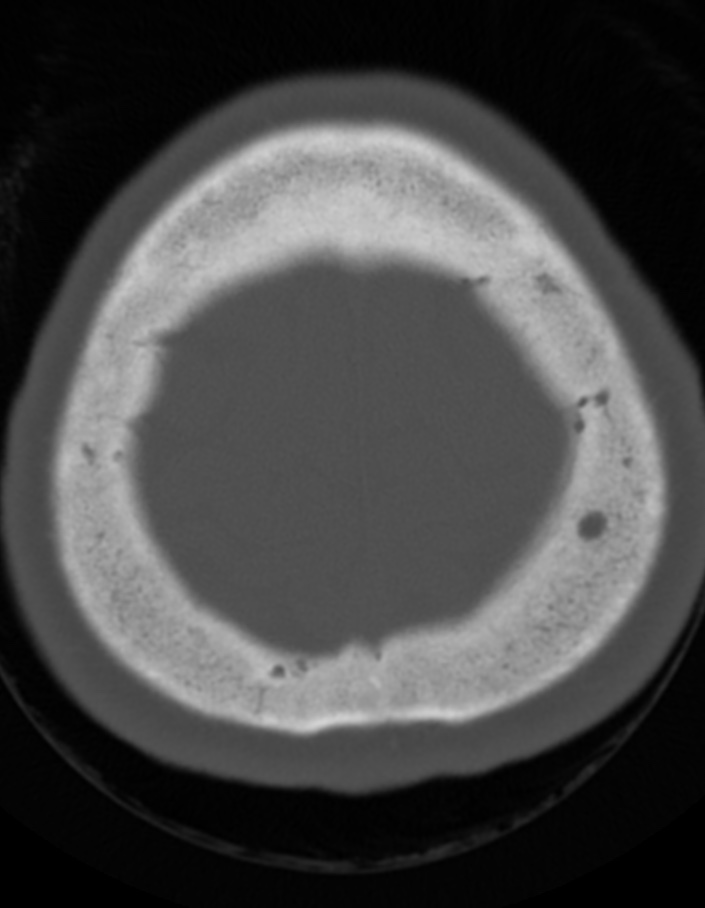
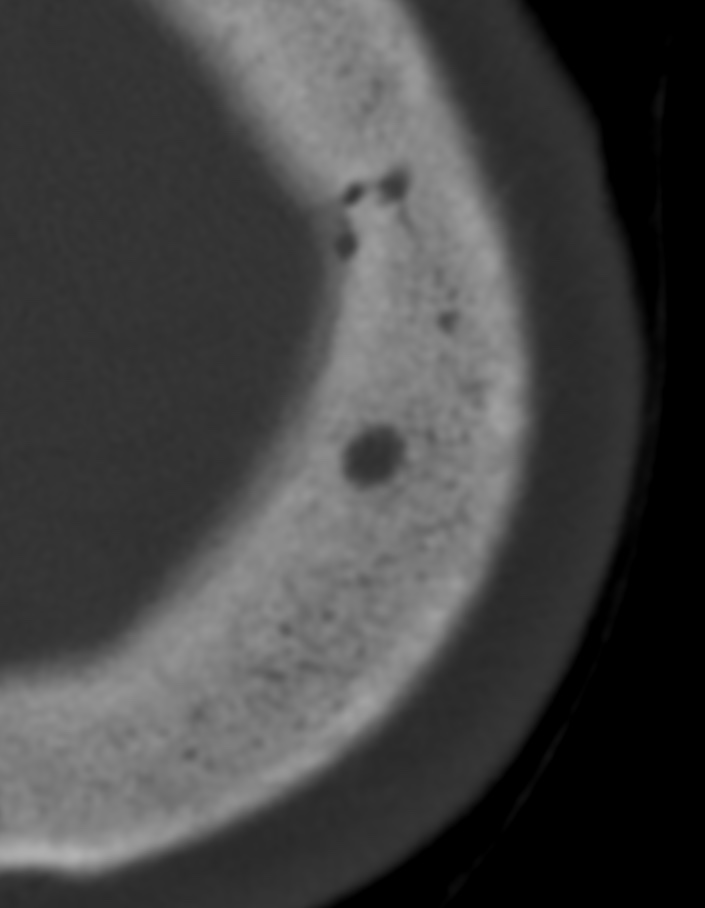
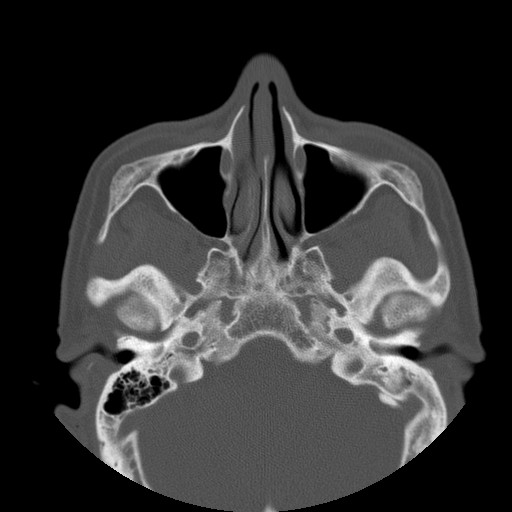
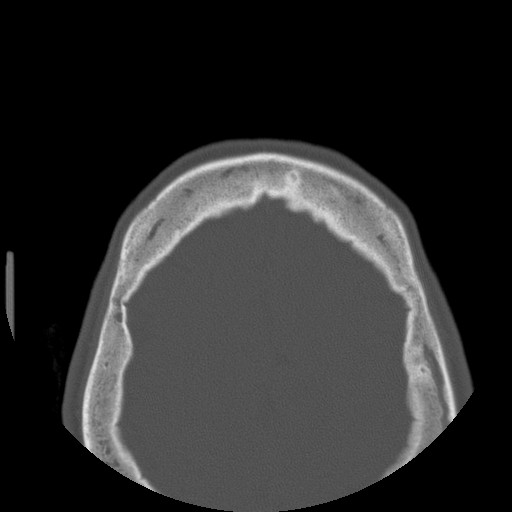
Calvarial lesions are uncommon and may constitute a diagnostic challenge. Pertinent clinical information such as patient age and history of trauma or underlying systemic disease should always be taken into consideration.
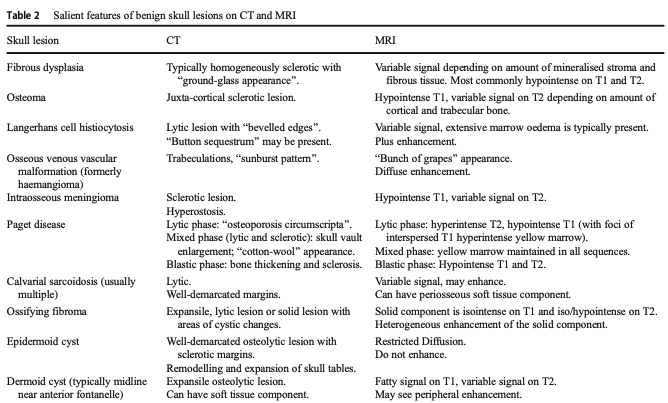
Among all imaging features, the extent, multiplicity, and attenuation of a calvarial lesion, in combination with knowledge of the patient’s age, are enough to narrow the differential diagnosis-
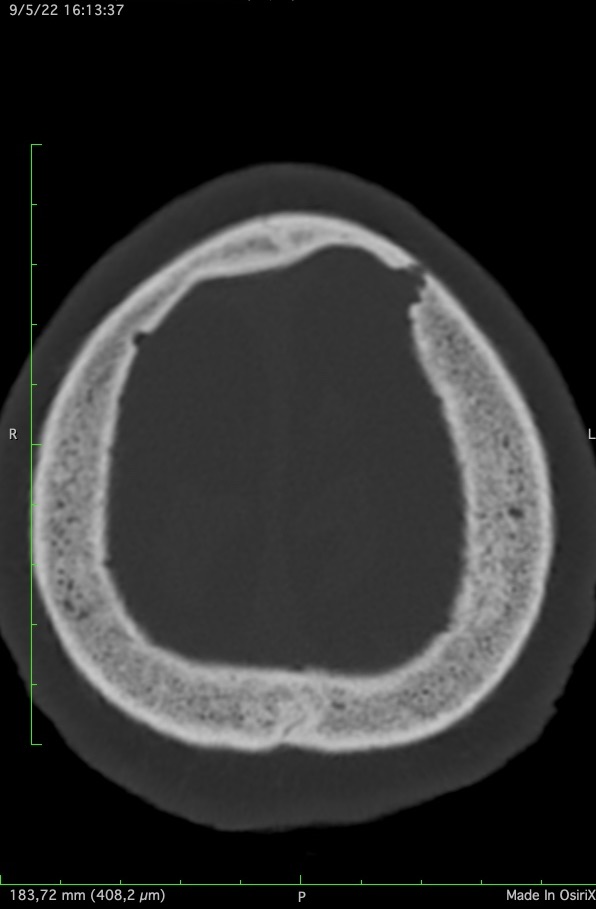
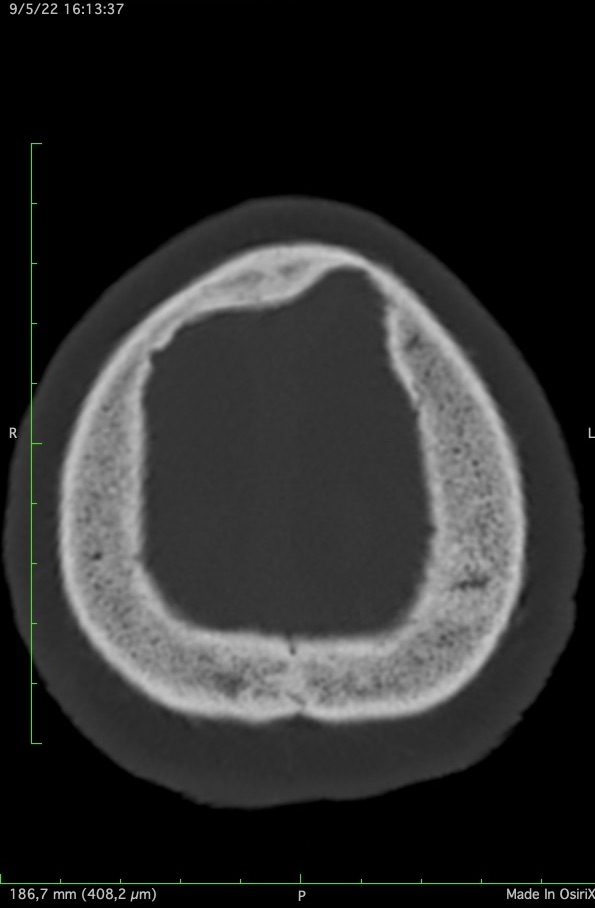
case 1
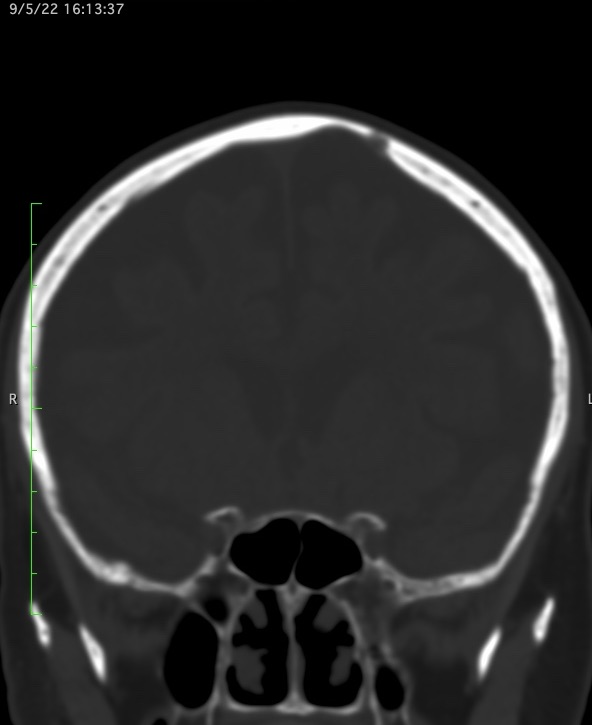
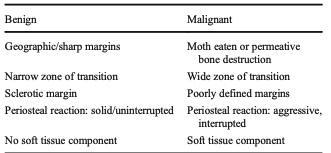
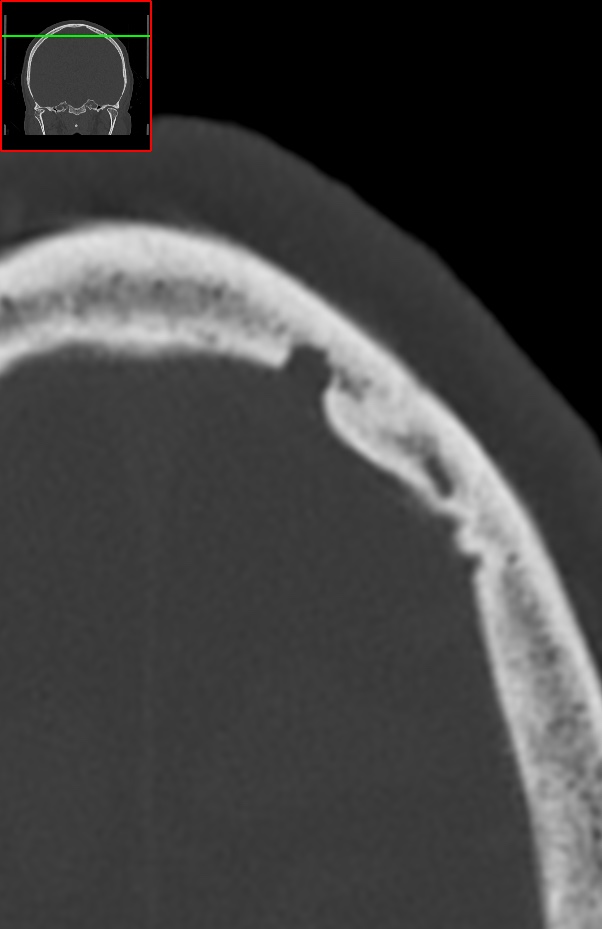
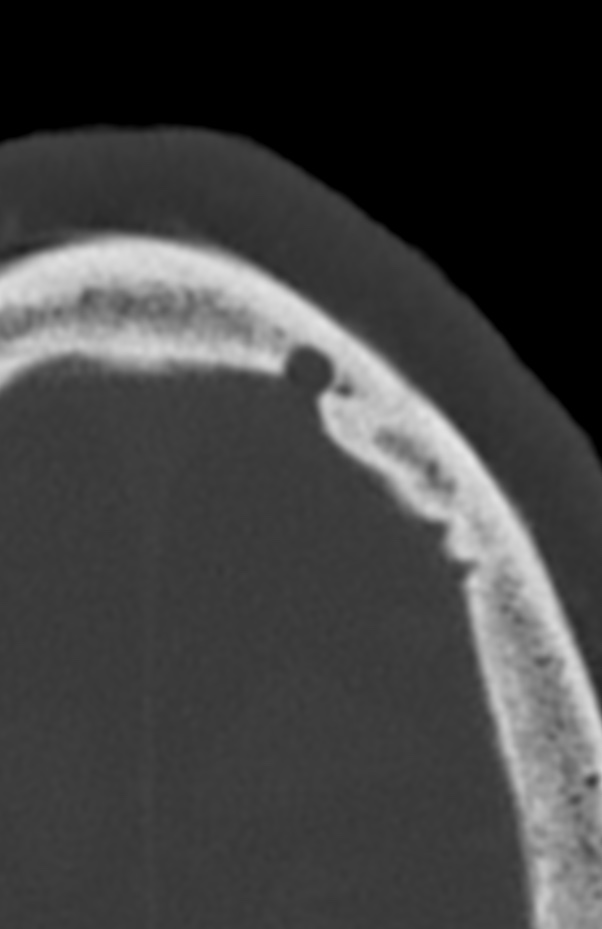
Recognition of benign and malignant imaging features is important for the radiological diagnosis. In general, benign tumours have well-defined borders with a narrow transition zone; sclerotic margins are frequently present. On the other hand, malignant tumours have poorly defined margins, a wide transition zone, aggressive periosteal reaction and often have a soft tissue component; these lesions cause dramatic bony destruction with intracranial or extracranial extension. Skull lesions can be lytic or sclerotic, single or multiple with varied composition; they may arise from osteogenic, chondrogenic, fibrogenic, vascular and/or other elements of bone.
80y Breast Cancer Follow up 2022case 264 ca mama. Paccionicase 4case 5case 5case 5case 6case 6Gallerycase 7 (trauma fracture c6/7)
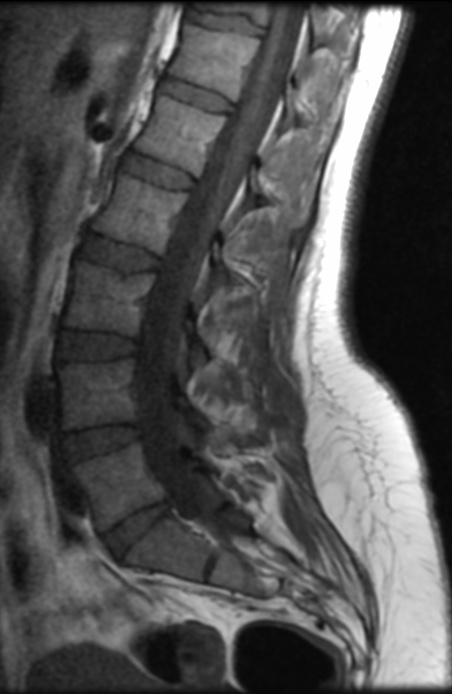
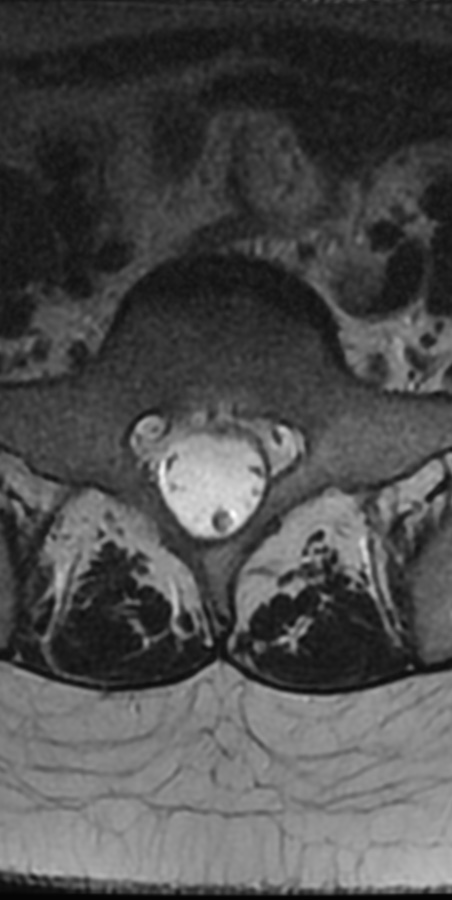
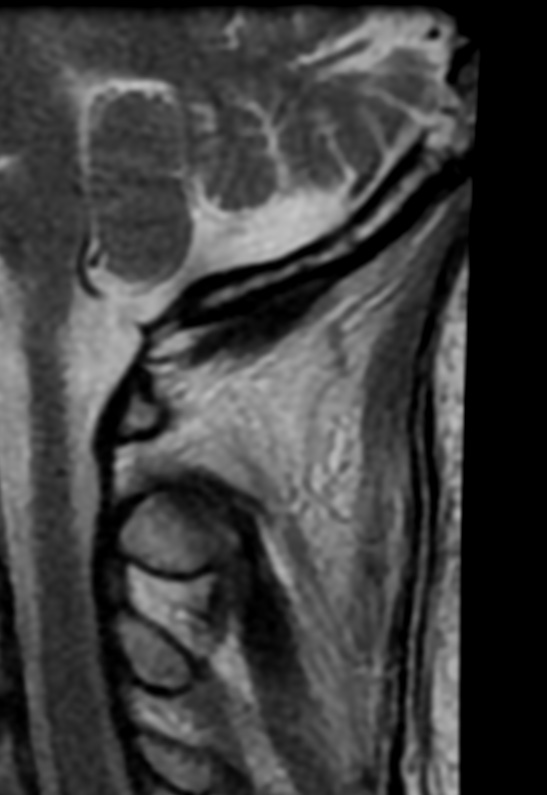
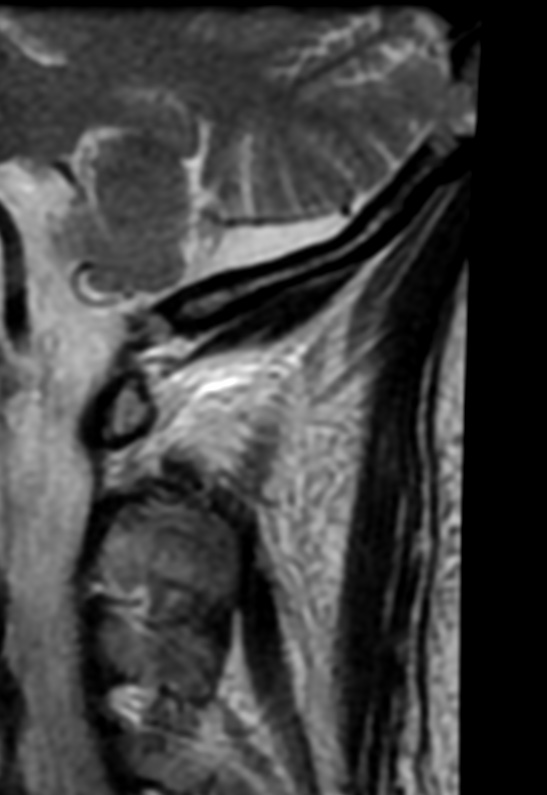
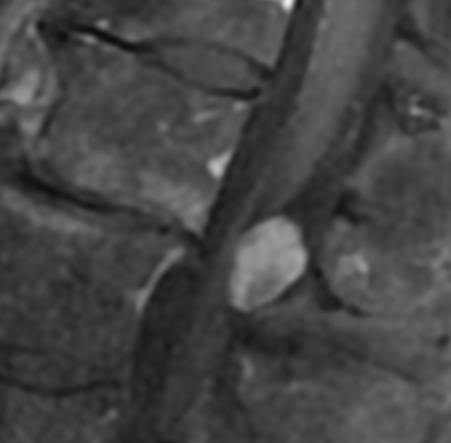
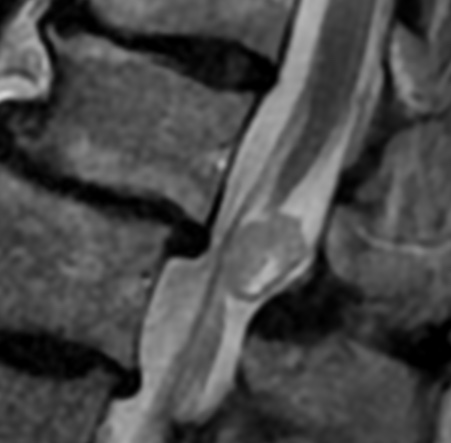
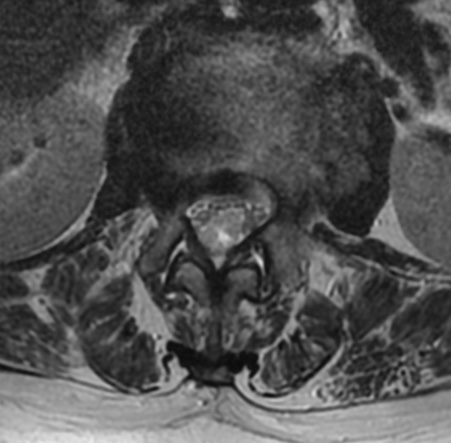
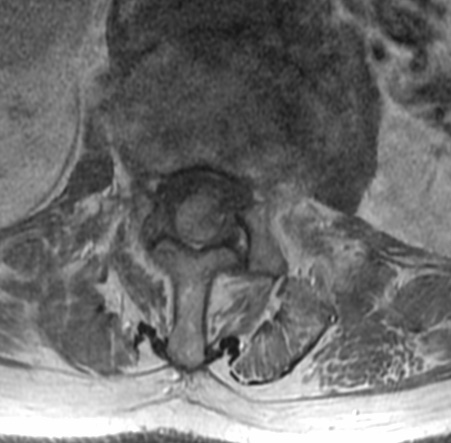
Spinal meningiomas, which are characteristically intradural and extramedullary, are relatively rare and account for less than 10% of all meningiomas and 25% of all spinal cord tumors.
Spinal meningiomas are intradural extramedullary lesions, usually benign, that are most commonly thoracic and posterolateral in location. Accounting for ~25% of spinal tumors, they are the second most common tumor in the intradural extramedullary location, second only to tumors of the nerve sheath. Most occur in middle-aged or older adults, with female predominance
Clinically, manifestations in patients with a meningioma of the lumbar spine depend on the tumor location, in relation to the spinal cord transection and nerve roots. Neurological symptoms include back or radicular pain, motor weakness, sensory disturbances, and urinary or fecal incontinence as a late finding.
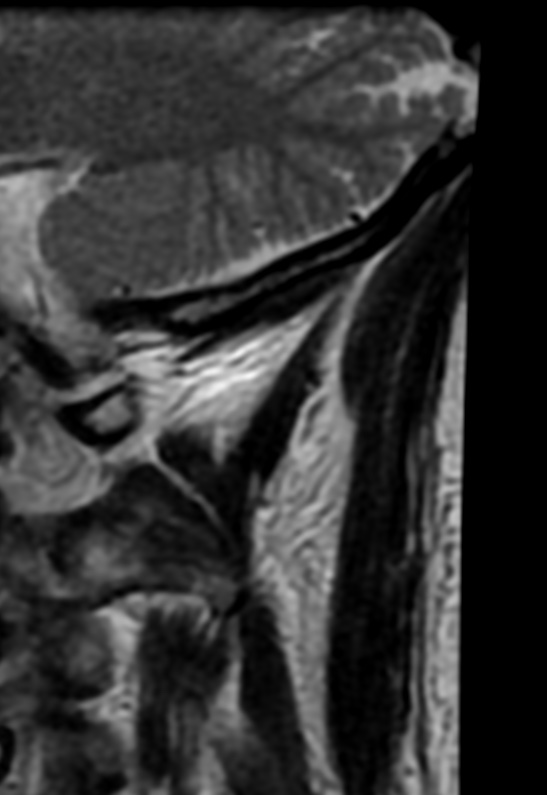
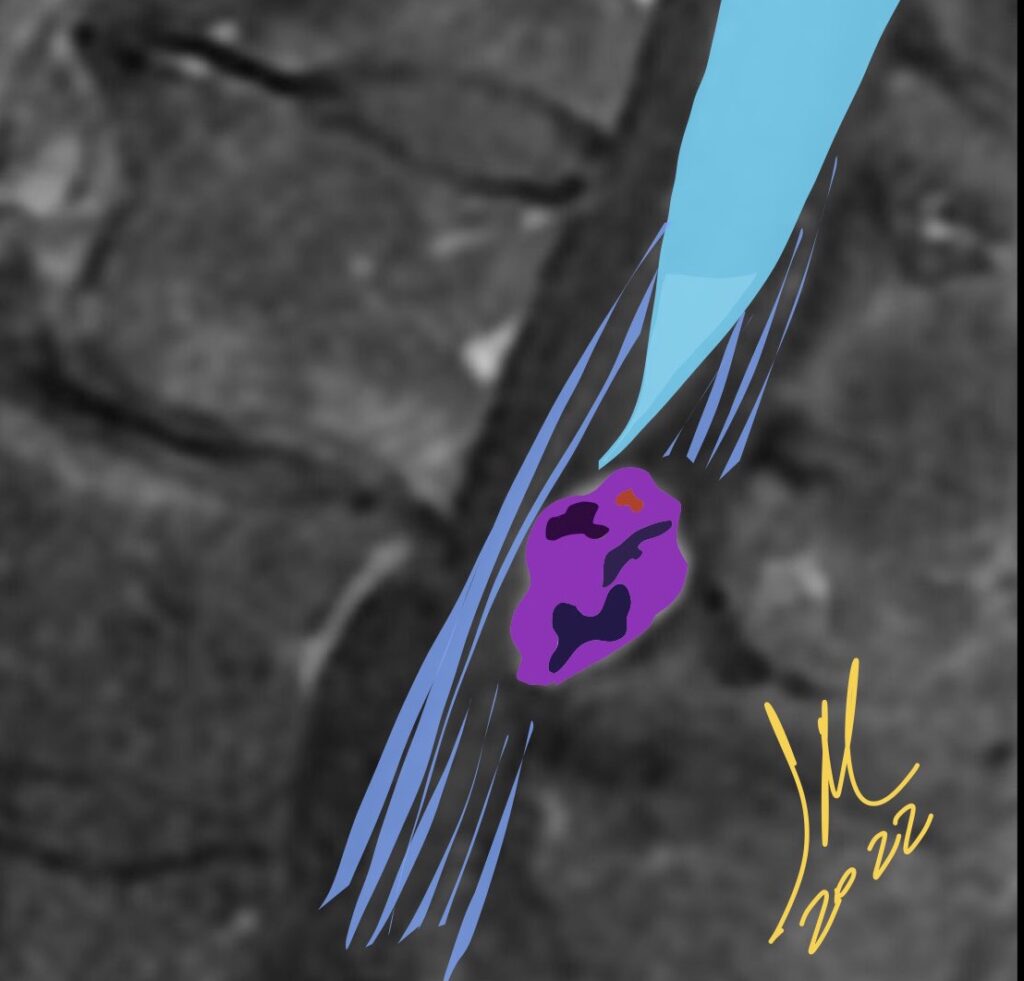
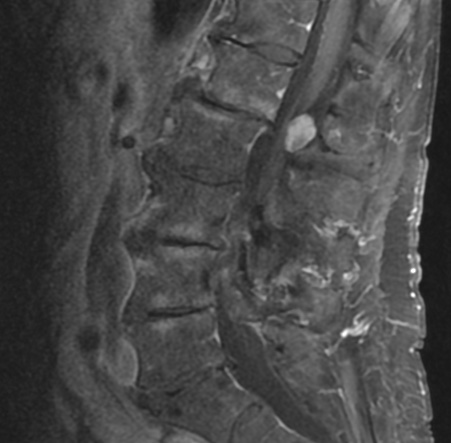
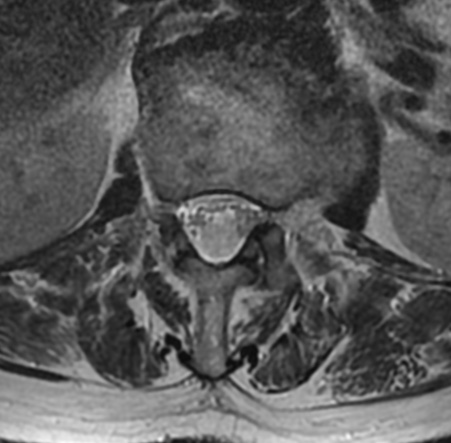
On MRI, characteristics of spinal meningiomas include well-circumscribed, broad-based dural attachment and/or a dural tail sign, which are similar signal characteristics to typical intracranial meningiomas. Spinal meningiomas typically demonstrate isointensity to slightly hypointensity on T1-weighted images, isointensity to slightly hyperintensity on T2-weighted images, and moderate homogeneous enhancement on T1-weighted images with gadolinium enhancement. Densely calcified meningiomas are sometimes hypointense on T1 and T2 images, and show only minimal contrast enhancement.
These radiological characteristics are usually nonspecific. It is difficult for physicians to differentiate benign or malignant tumors simply on images. The “dural tail sign”, for example, can be seen in intradural-extramedullary meningiomas but is also found in metastatic tumors and lymphomas.
A meningioma with intradural and extradural components occasionally mimics a nerve sheath tumor and a nerve sheath tumor with a predominant intradural component may mimic a meningioma; however, nerve sheath tumors are usually hyperintense on T2, lumbar and ventral in location, rarely calcified, more common in men, and do not have a dural tail
Reference:
Yeo Y, Park C, Lee JW, et al. Magnetic resonance imaging spectrum of spinal meningioma. Clin Imaging 2019; 55:100-106
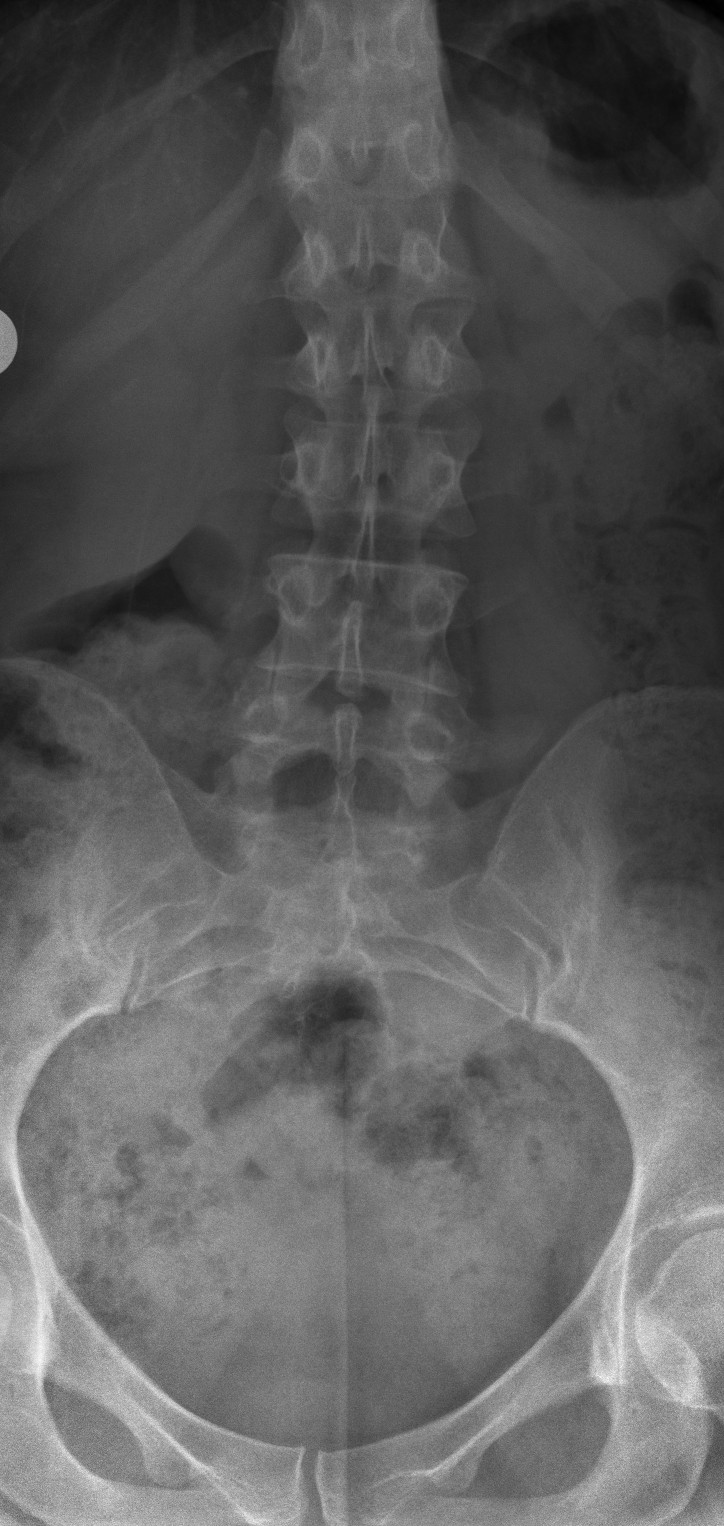
Acromegaly is a chronic and slowly developing disease caused by hypersecretion of GH and consequently of IGF-I.
The spine, noticeably targeted by chronic GH excess, presents widened intervertebral spaces, vertebral enlargement, and osteophyte formation, which are caused by endocondral, marginal, and subligamentous growth of vertebral bone.
The hyperostotic changes may be so relevant as to resemble to those observed during the diffuse idiopathic skeletal hyperostosis (DISH) syndrome.
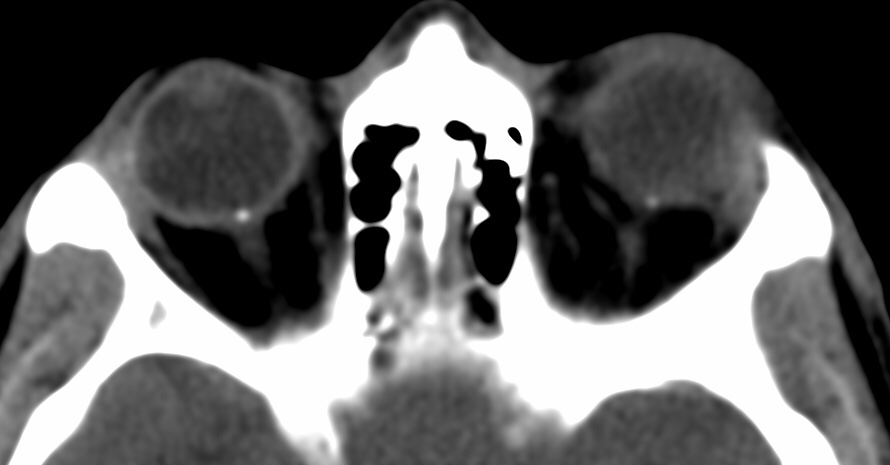
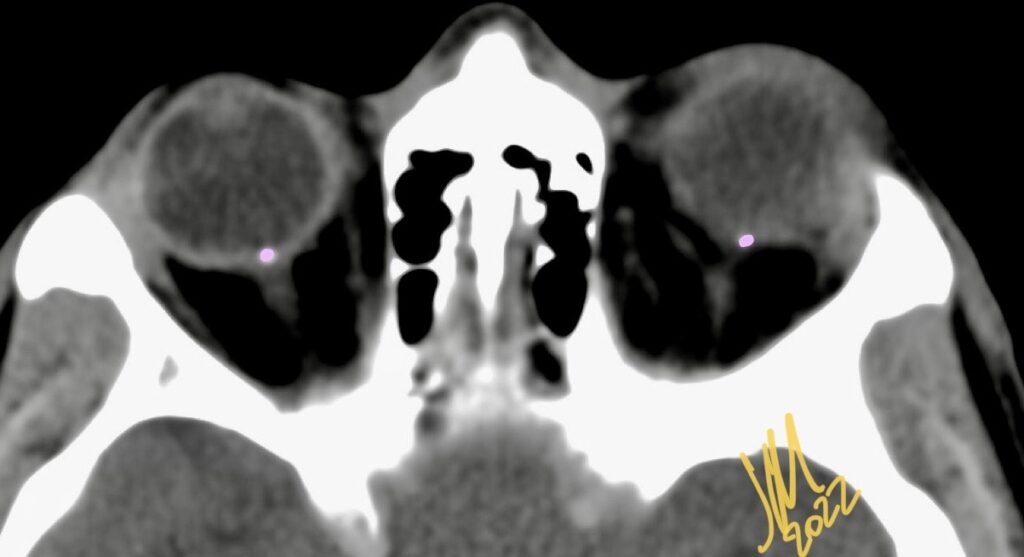
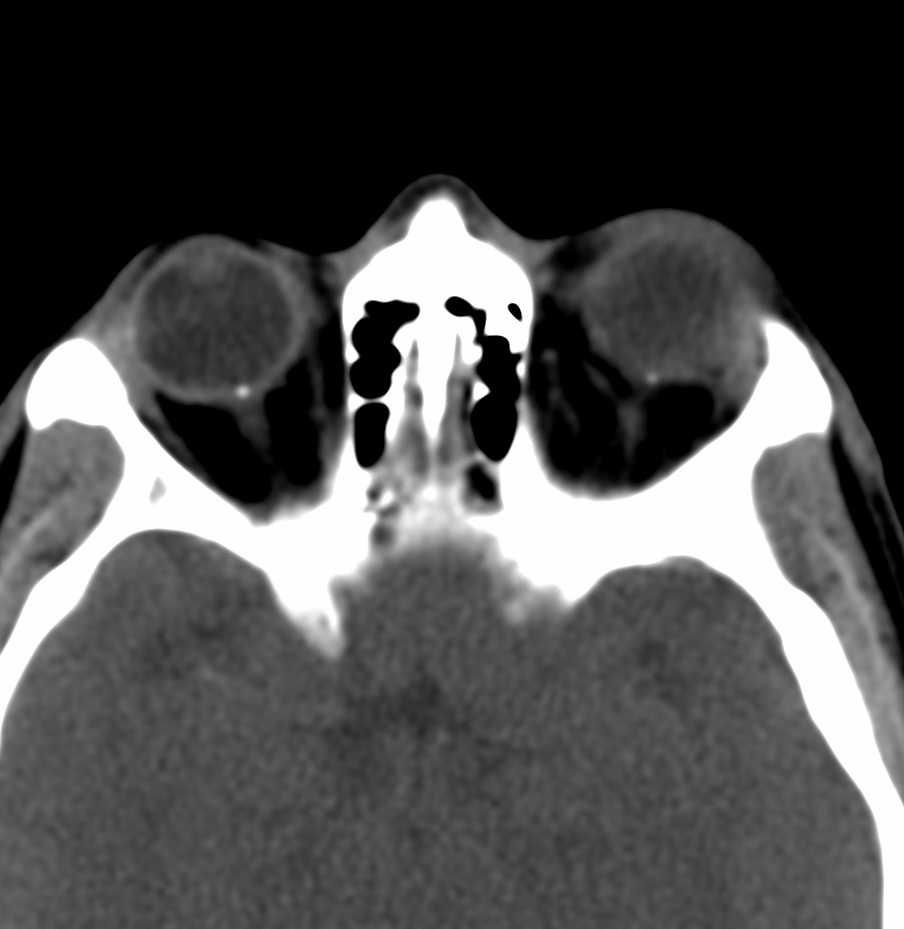
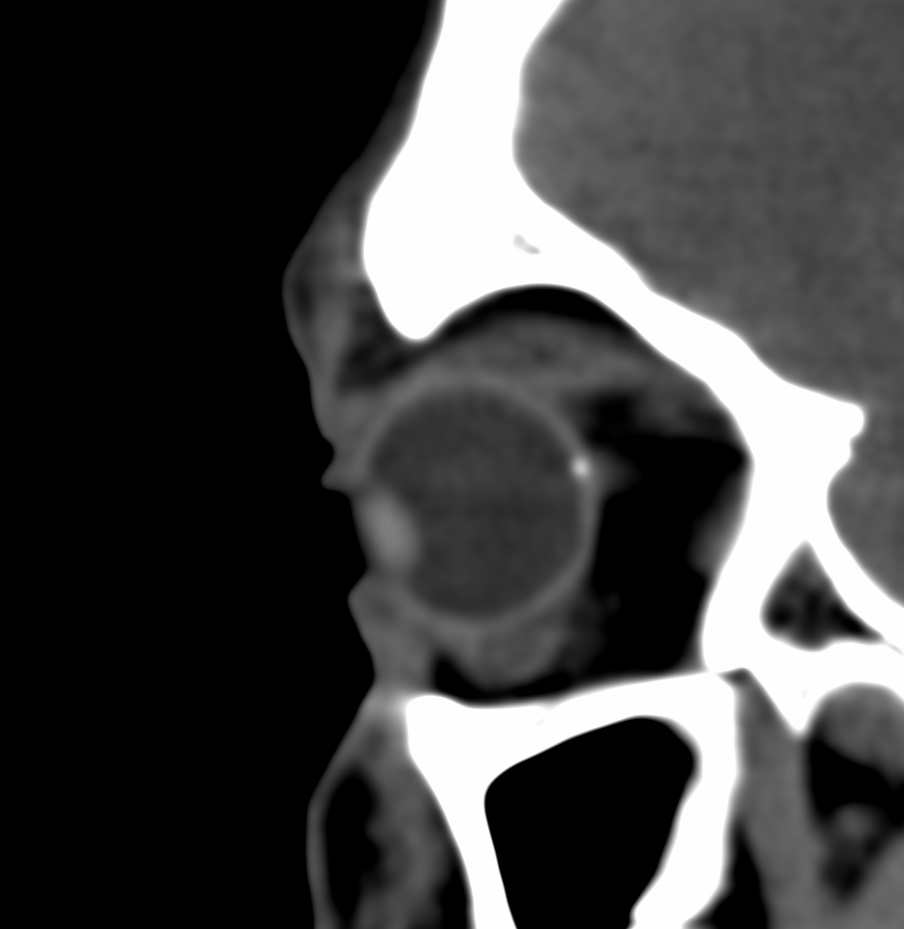
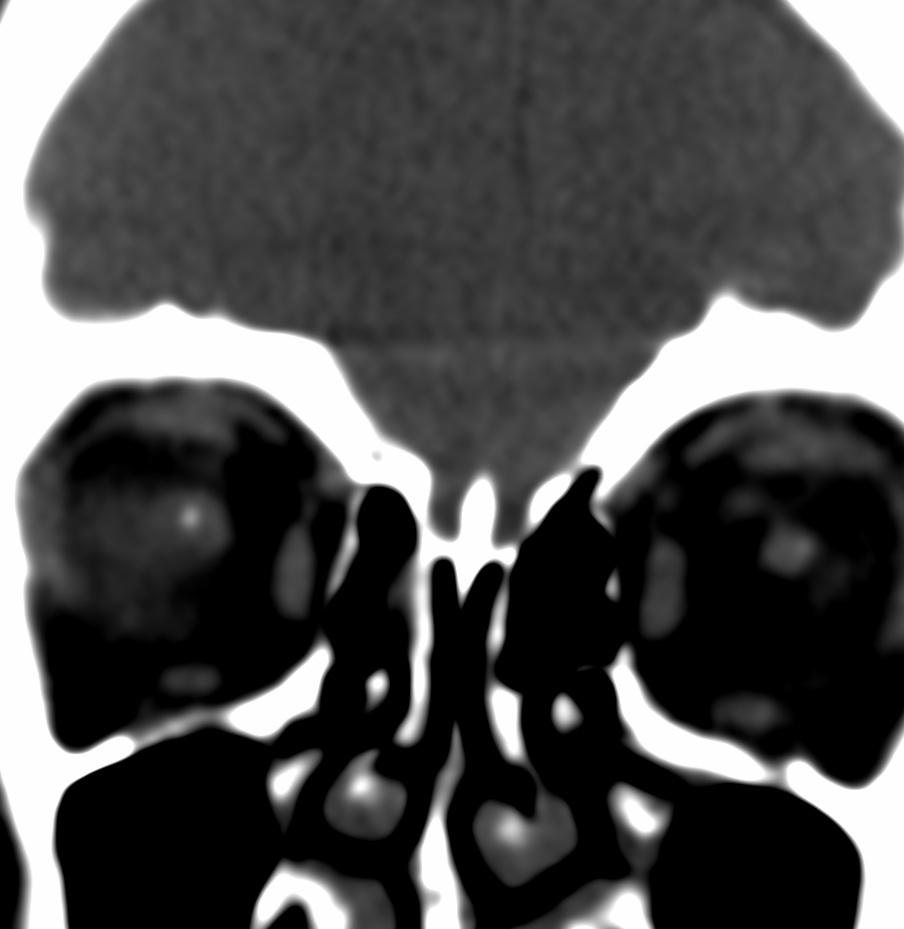
Drusen are a rare inherited pathology , usually bilateral and asymptomatic, but they can lead to a visual field defect or to migraine-like headaches.
Drusen are classified into two categories: retinal and optic disc.
A benign calcification at the optic nerve head junction affects 0.25%-2.0% of the population and is more prevalent in White people. The condition is a result of acellular calcific deposition within the optic nerve that may mimic papilledema on fundoscopic exam, thus representing a diagnostic challenge for clinicians.
Reference:
Kumaev B, Soule E, Rao D, Fiester P. Optic Disc Drusen. Appl Radiol. 2020;49(6):54-55.
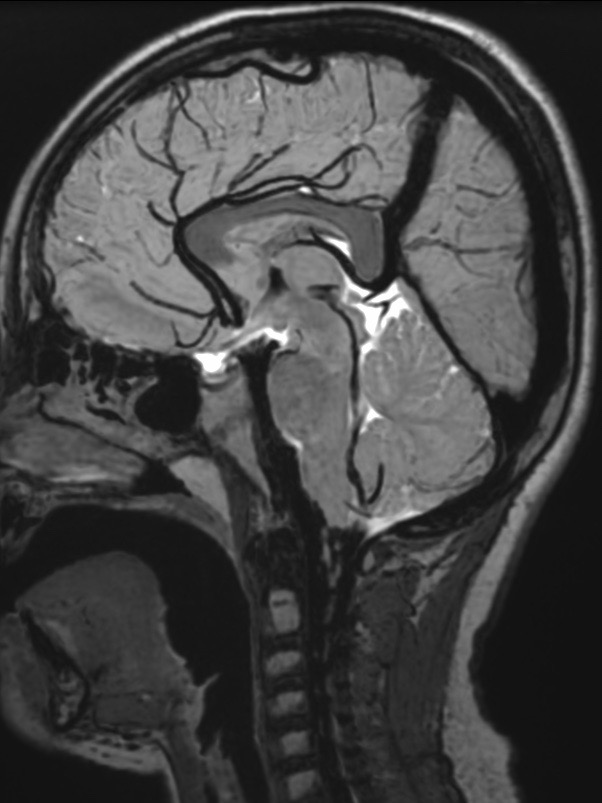
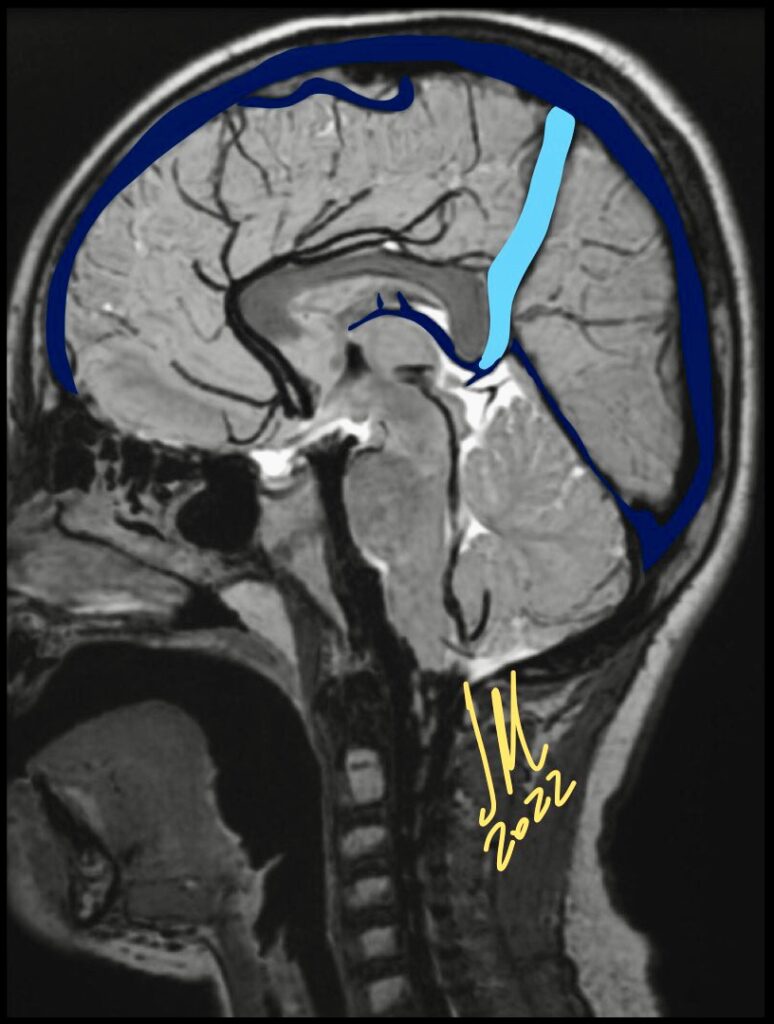
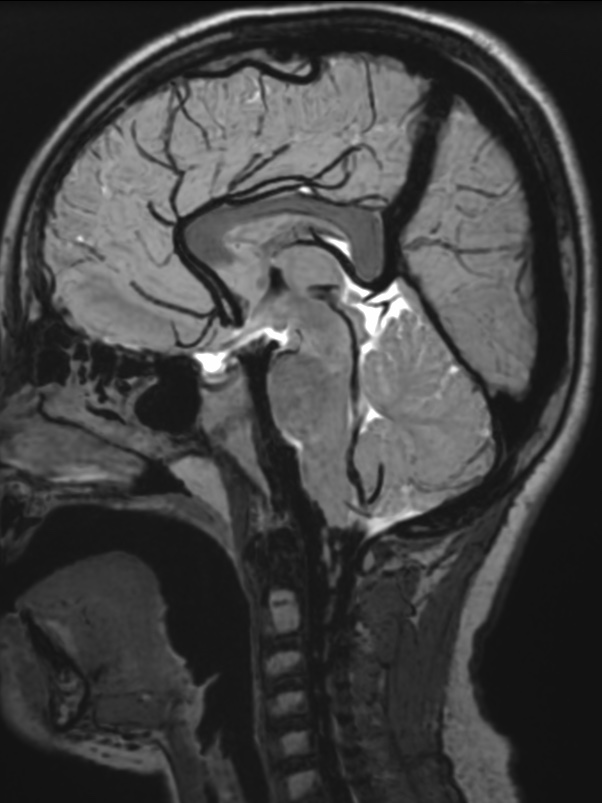
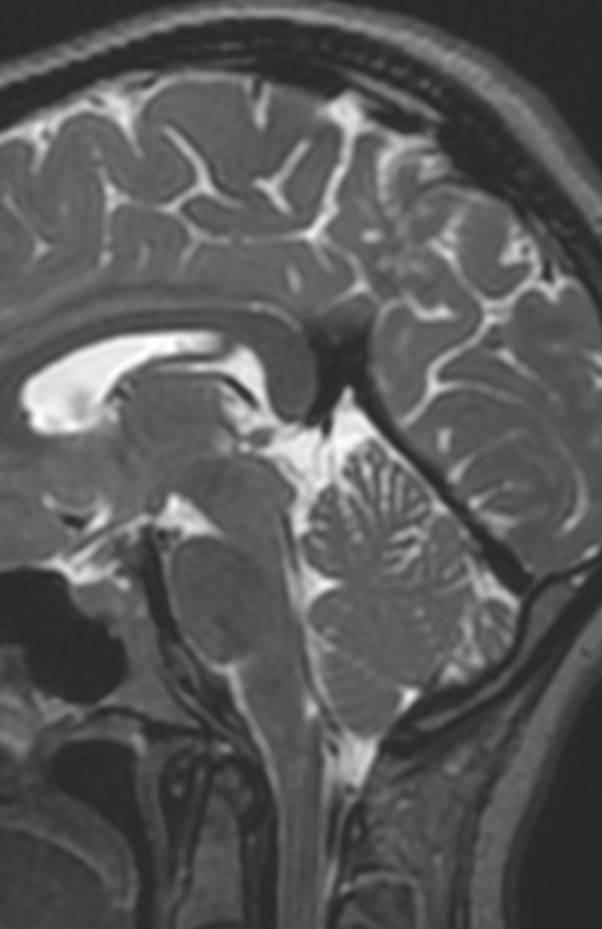
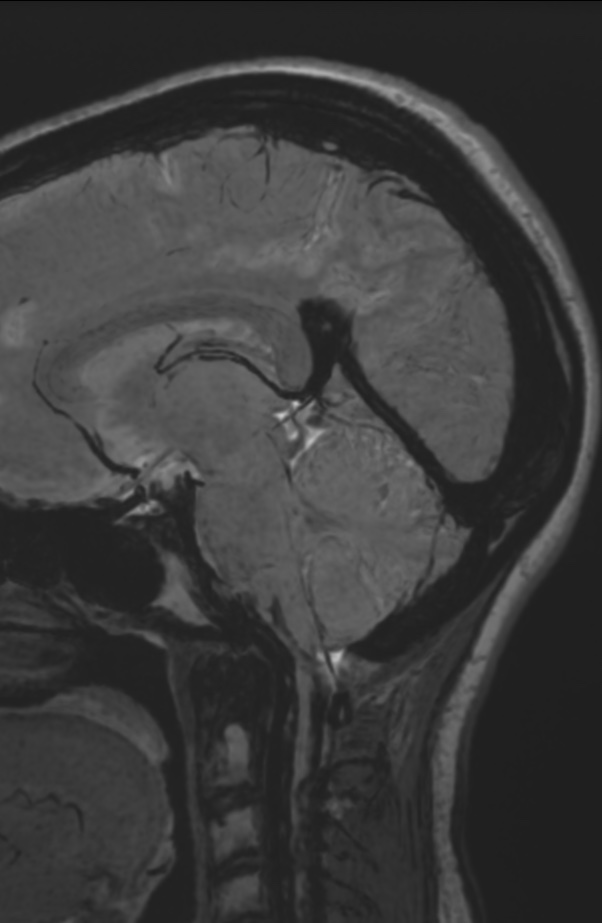
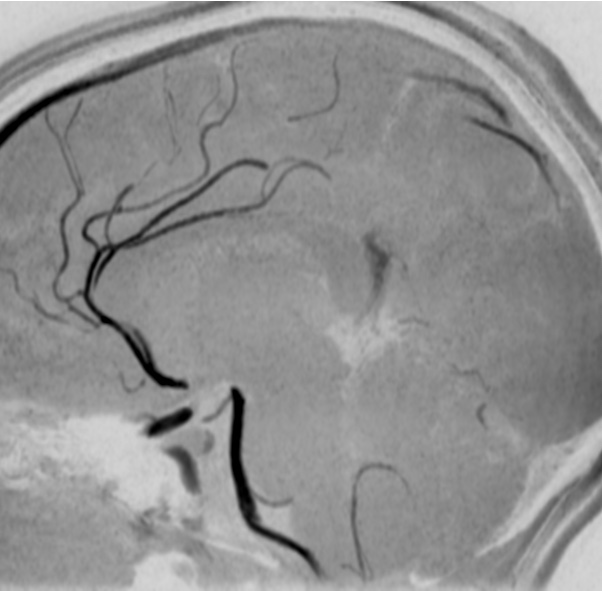
Persistent falcine sinuses are exceptionally rare and are typically present in the context of absent, hypoplastic, or occluded venous outflow tracts.This observation implies that alterations in cerebral venous flow dynamics may result in recanalization of the falcine sinus.
The falcine sinus is an embryonic venous structure in the falx cerebri that connects the vein of Galen to the superior sagittal sinus.
It normally closes before or shortly after birth. Persistent falcine sinus can be a congenital or acquired phenomenon related to a defect in the straight sinus that is thought to cause an alternative pathway to form for drainage from the deep to superficial venous system.
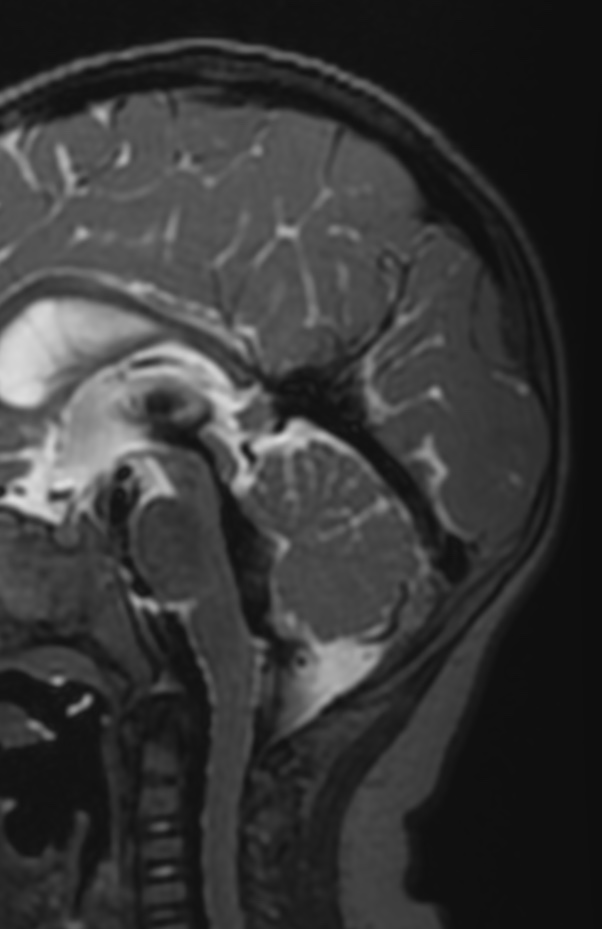
1Y. Hypoplasia1Y. hypoplasia
The falcine sinus normally closes before or shortly after birth. Congenital persistence of the falcine sinus is believed to be caused by a mesenchymal disorder that can also lead to hypoplasia or absence of the straight sinus. It may or may not be associated with other congenital anomalies of the brain.
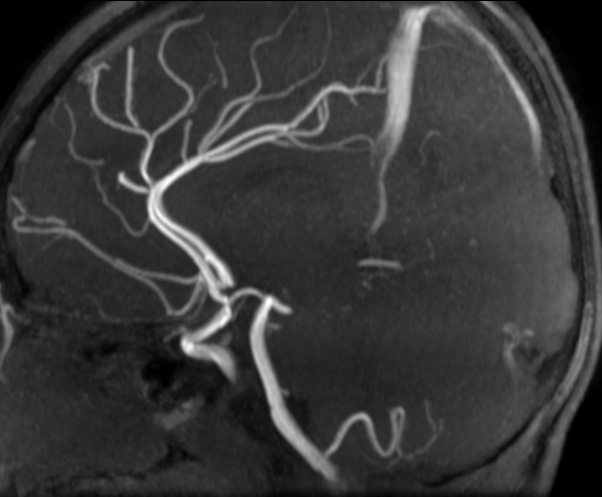
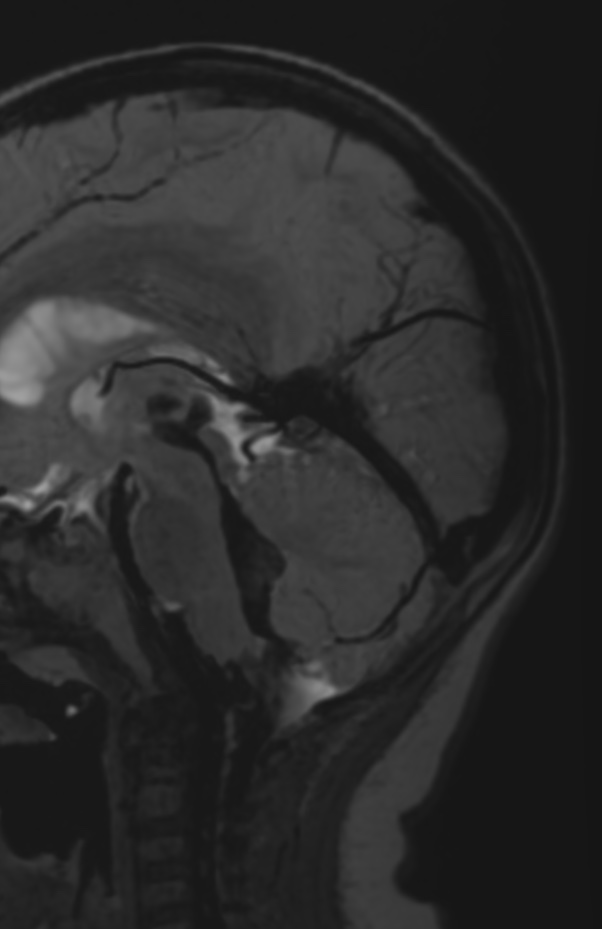
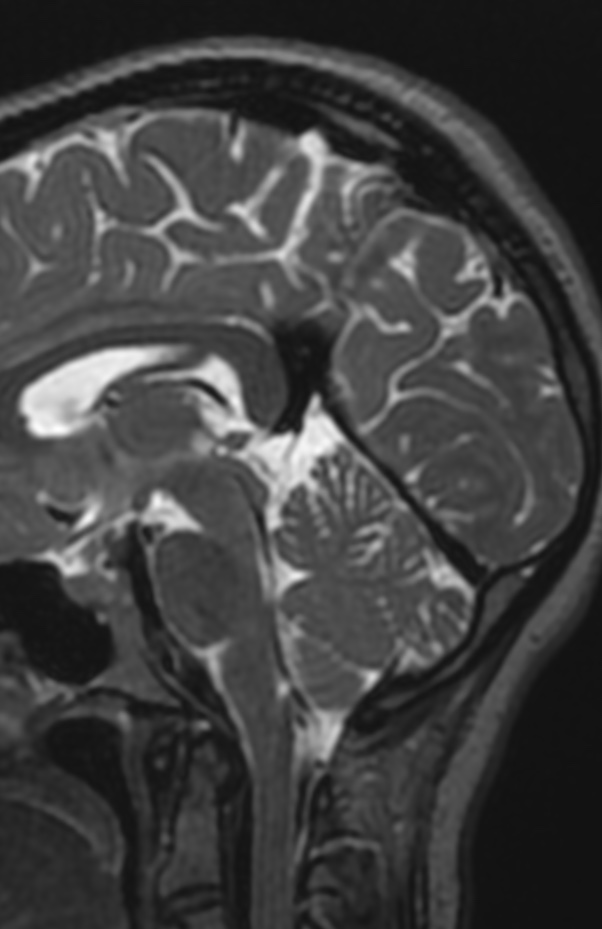
Alternatively, persistent falcine sinus can be an acquired phenomenon with recanalization after thrombosis or obstruction of the straight sinus.
30Y Atresia30M Atresia
Once a persistent falcine sinus is identified, a thorough search for additional findings is imperative given the importance of early intervention in the developing brain.
Reference:
American Journal of Neuroradiology December 2020, 41 (12) 2351-2357; DOI: https://doi.org/10.3174/ajnr.A6816
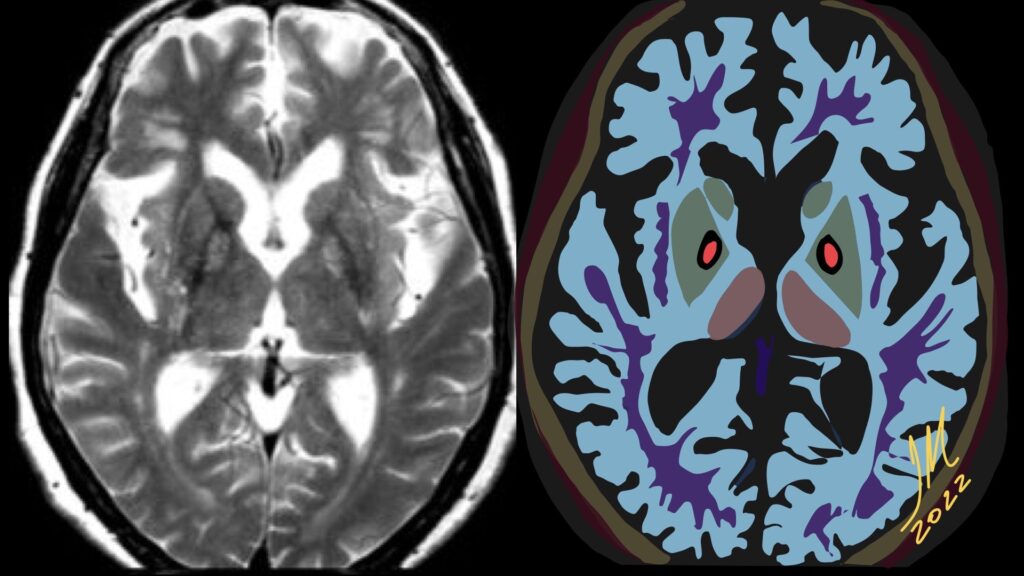
Hallervorden-Spatz disease now known as pantothenate kinase-associated neurodegeneration is a rare autosomal recessive neurodegenerative disorder associated with iron accumulation in the brain nuclei and characterized by progressive extrapyramidal dysfunction and dementia.
Is the standard in the diagnostic evaluation of all forms of Neurodegeneration with brain iron accumulation. It has significantly increased the likelihood of a diagnosis of PKAN.
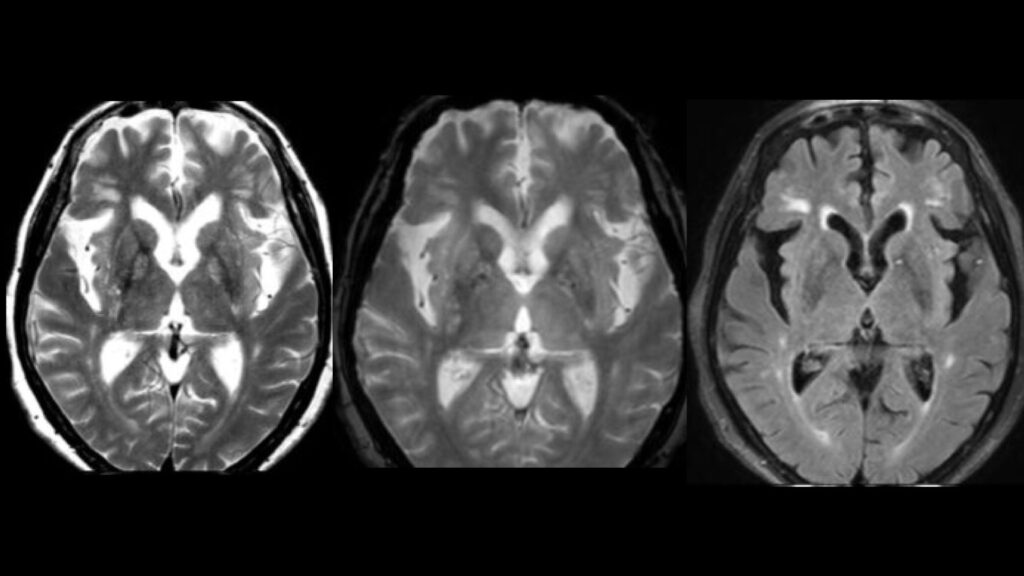
Imaging findings are most conspicuous on T2W-SWI-GRE sequences which demonstrate hypointensity reflecting areas of iron deposition, mainly in globi pallidi, pars reticulata of the substantia nigra, and red nuclei.
Studies report that all patients with PANK2 mutations, whether classic or atypical, have the characteristic radiologic sign known as «eye of the tiger» on brain MRI, which is evident as bilateral symmetrical, central foci of hyperintense signals in the anteromedial globus pallidus, with surrounding zone of hypointensity in the globus pallidus on T2W MR scanning. The central T2 relatively hyperintense spot or line within the globi pallidi is due to gliosis and vacuolation.
This sign was not reported in patients without PANK2 mutations. Cortex is usually spared, but atrophy can be seen in advanced cases. SWI-GRE Show susceptibility artifact (blooming low signal) in corresponding areas due to iron accretion. MR spectroscopy shows decreased NAA peak due to neuronal loss and may depict increased myoinositol.
Patients with mutations in the PANK2 gene can be distinguished from patients without the mutation by their specific brain MR imaging changes, even very early in disease.
Reference:
S.J. Hayflick, M. Hartman, J. Coryell, J. Gitschier and H. Rowley. American Journal of Neuroradiology June 2006, 27 (6) 1230-1233;
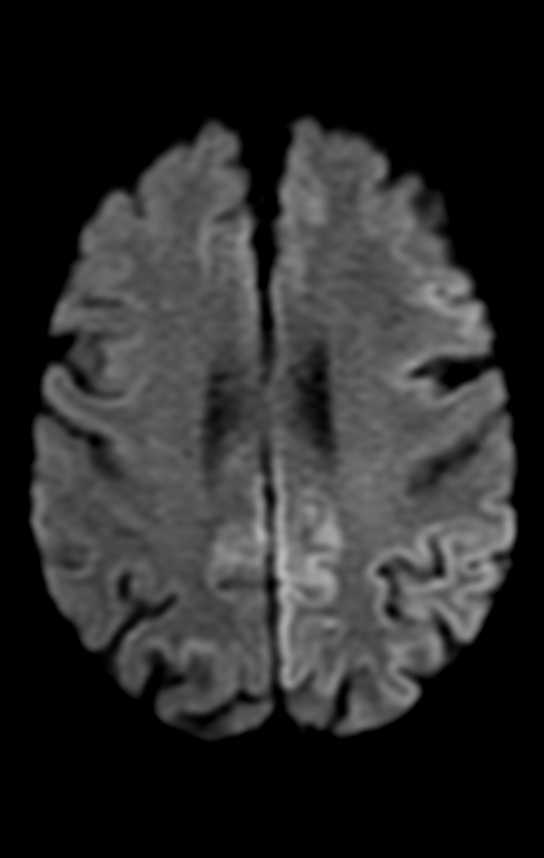
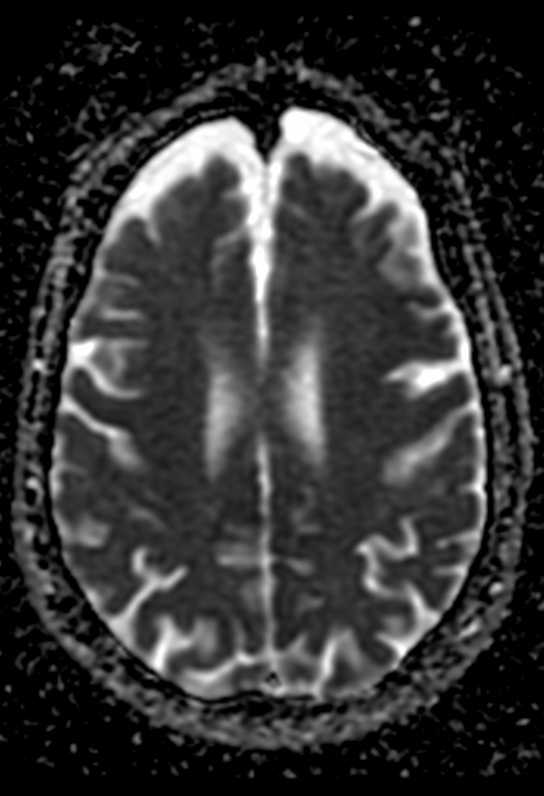
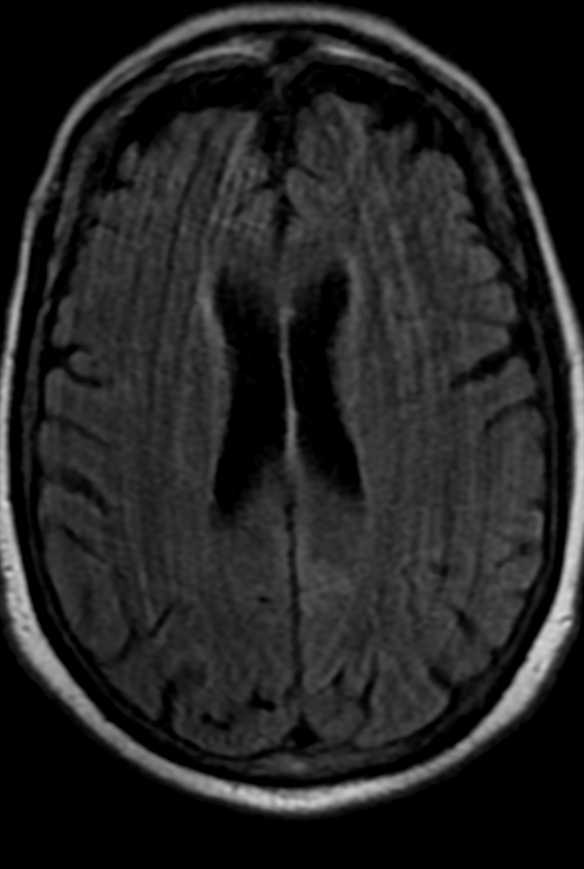
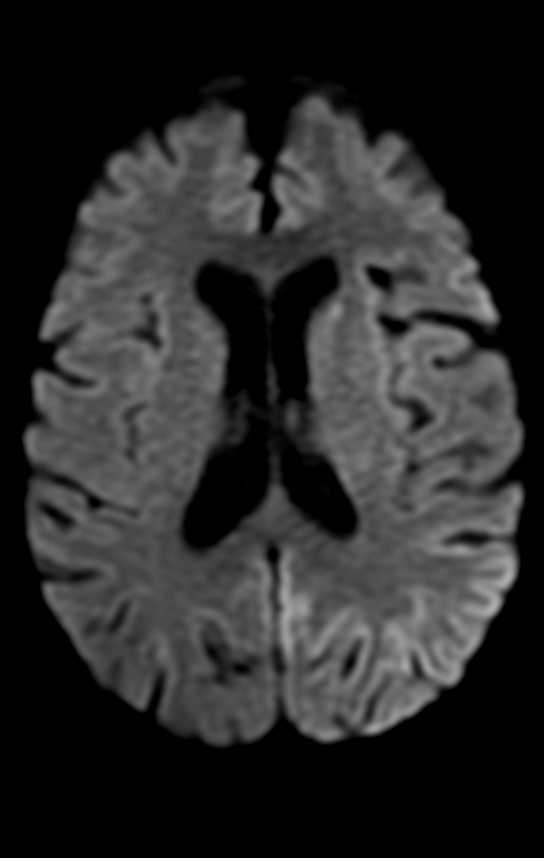
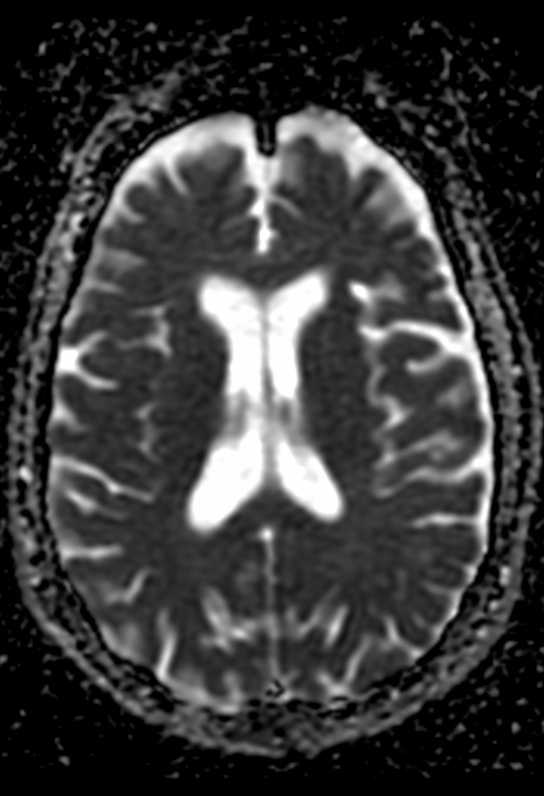
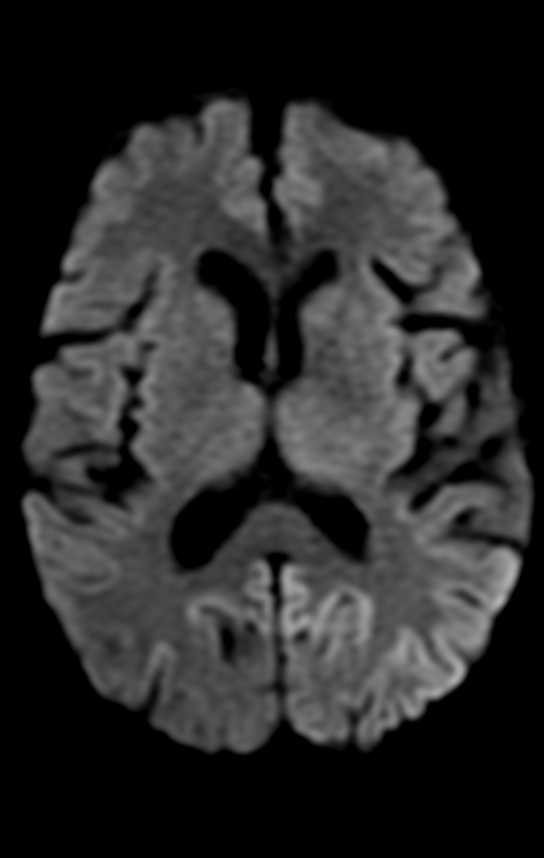
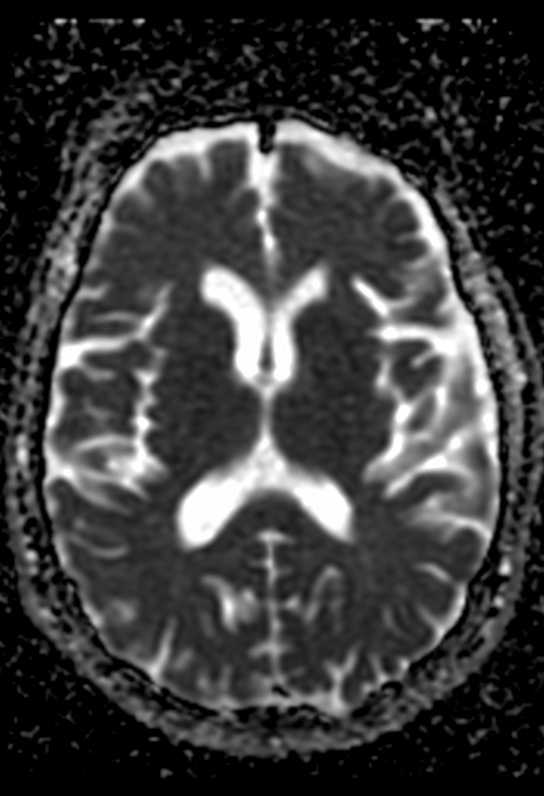
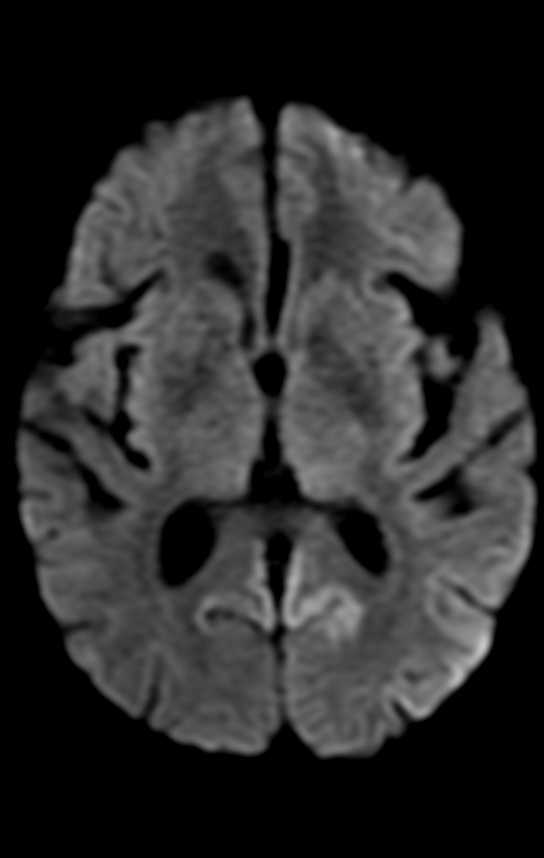
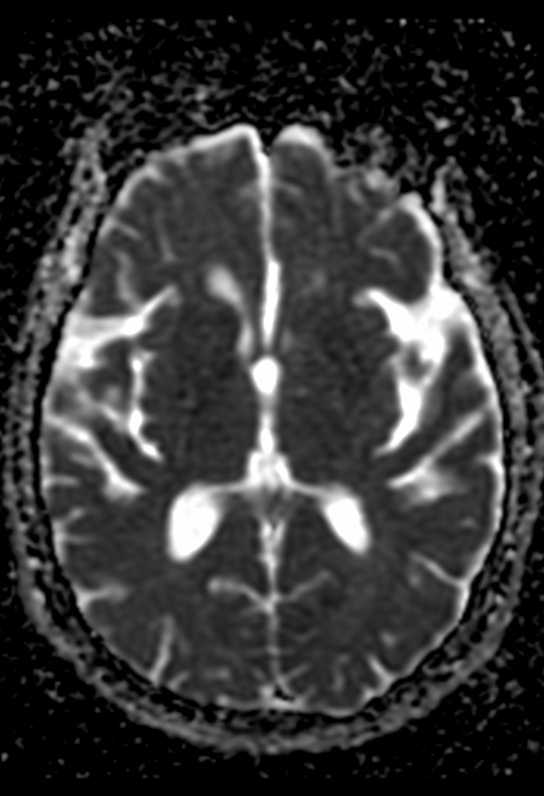
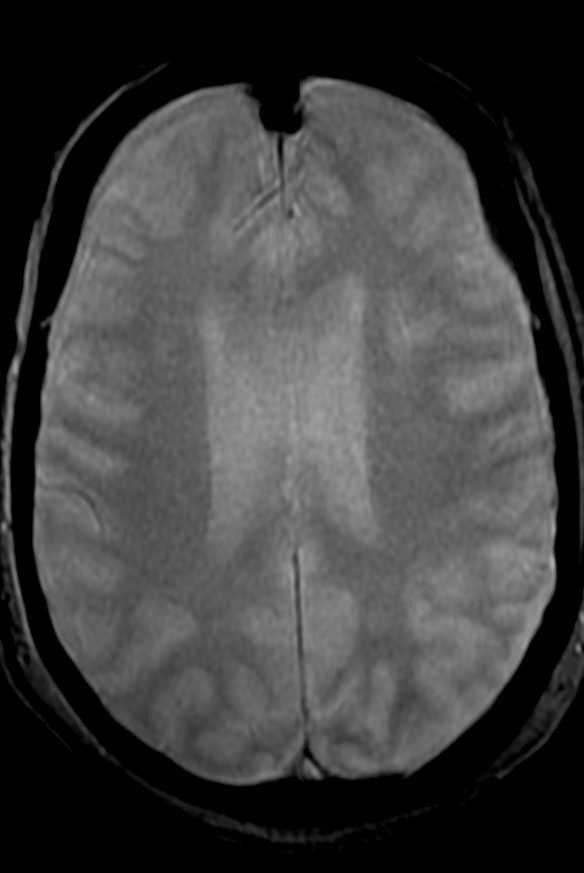
On MR imaging, the earliest changes are seen on DWI sequences. The involved regions show restricted diffusion with corresponding ADC hypointensity. The extent of these abnormalities depends on severity and duration of hypoglycemia.
Changes are usually bilateral, though bilaterally asymmetric, or, rarely, unilateral lesions, may occur. Reduction in ADC values has been shown to follow establishment of cerebral isoelectricity, a process that may be asynchronous. This may explain asymmetric lesions in a given patient.
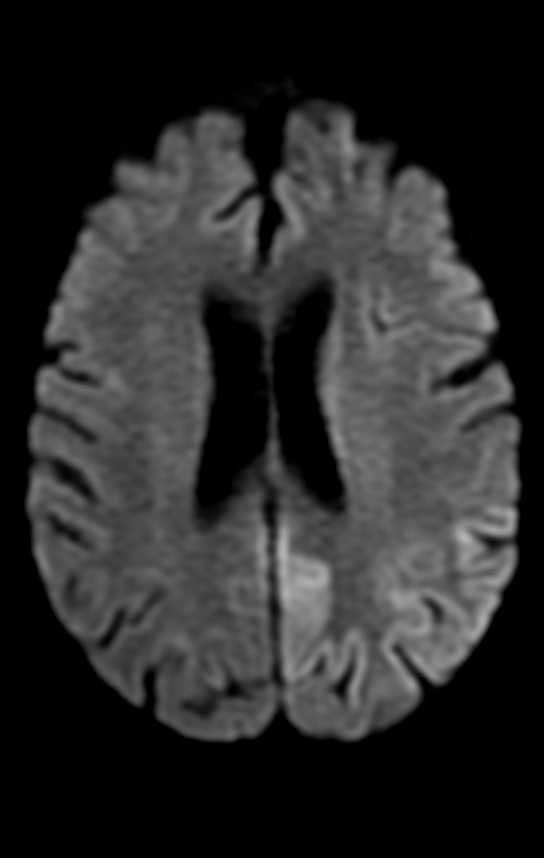
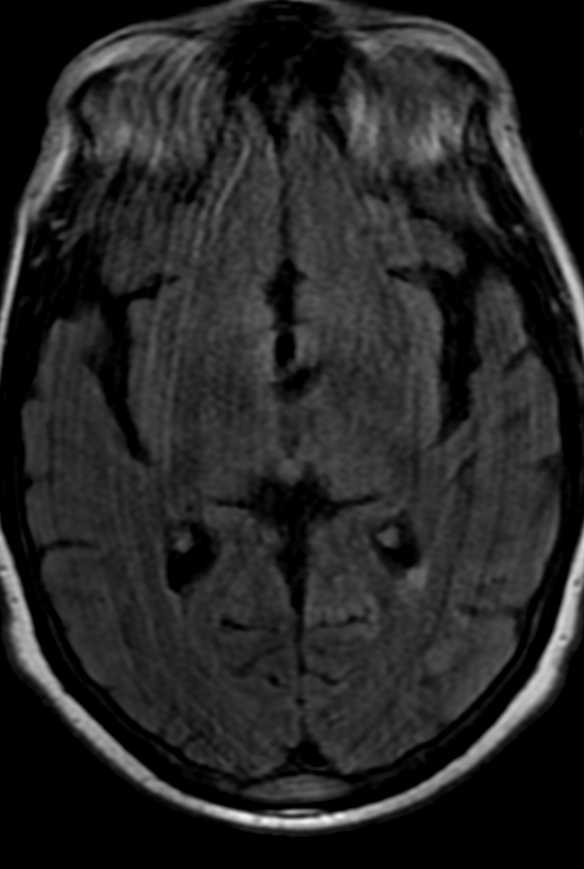
On the basis of the topographic distribution of the signal abnormalities, 3 imaging patterns have been described. These include 1) predominant gray matter involvement affecting the cortex, neostriatum, and hippocampi; 2) predominant WM involvement affecting the periventricular WM, internal capsule, and splenium of corpus callosum and 3) mixed pattern, involving both the gray matter and WM.
The division of patients on the basis of these imaging patterns is of unclear significance.Patients with focal involvement of the internal capsule, corona radiata, or splenium usually have a good prognosis. These lesions usually resolve promptly after restoration of blood glucose, though they tend to follow clinical symptom resolution. Resolution of DW abnormalities in their patient as early as 2 hours after blood glucose levels were restored.
Patients with extensive WM involvement show variable response. The prognosis in these cases varies between complete recovery and persistent vegetative state. Clinical improvement, if it occurs, is usually delayed by weeks.Involvement of the neostriatum and diffuse cortical lesions often portend dismal outcome. Failure of lesions to regress on follow-up imaging is also associated with poor prognosis.
Findings of CT scans of the head on admission were often unremarkable in the reported cases, but in time, some acute-stage and chronic-stage changes have been demonstrated. In the acute stage, the changes varied from subtle decreased attenuation of the basal ganglia to diffuse brain edema, as severity of the hypoglycemia increased. In the chronic stage, diffuse brain atrophy and dilation of the ventricular system have been noted. MR imaging findings are comparable to the CT findings, mainly involving the cortex, internal capsule, basal ganglia, and hippocampus.
Diffusion-weighted MR imaging detects change in water diffusion with cellular dysfunction and primarily identifies early ischemic changes in stroke. Infarction is the most common cause of such a hyperintense lesion on diffusion-weighted imaging. In hypoglycemia, the incidence of cytotoxic edema, shrinkage of the extracellular space as a result of hypoglycemia, and failure of the ionic pumps cause the hyperintense lesion on diffusion-weighted MR imaging. ADC reductions similar to those seen after ischemia occur in hypoglycemia, status epilepticus, spreading depression, and excitotoxic brain injury, pathologic conditions characterized by a significant shrinkage of the extracellular space volume. However, status epilepticus and spreading depression in normal brain are conditions that are not associated with energy failure, and the ADC changes are reversible. Glucose deprivation leads to severe brain energy failure and a reduction of cell membrane ionic pump activity, as does anoxia/ischemia, but the topographic and temporal evolution of hypoglycemic brain damage is different from that of anoxia/ischemia.
Hyperacute short-term severe hypoglycemia for <10 minutes does not induce visible changes in DWI of the human brain, suggesting that prolonged hypoglycemia may be the relevant cause for observed reversible diffusion disturbances in MR imaging. Therefore, prompt adequate therapy for hypoglycemia can prevent cerebral injury in patients with diabetes.
Hypoglycemia was initially reported to predominantly involve the cortex, neostriatum, and hippocampus.However, many authors have also reported predominant WM involvement, mainly affecting the centrum semiovale, corona radiata, internal capsule, an splenium of the corpus callosum.In fact, involvement of the WM is now thought to be earlier and more common than gray matter involvement. Some cases may show diffuse gray matter and WM involvement. The thalamus, brain stem, and cerebellum are invariably spared, and this may help to differentiate hypoglycemia from hypoxic injury, which often involves the thalamus.
Hypoglycemia is more common in diabetic patients and can occur as a complication of therapy with insulin or long-acting sulfonylurea drugs. Other causes include exogenous administration of insulin, which may be suicidal or accidental, insulin-secreting tumors, sepsis, Addison disease, and hepatic or renal failure.