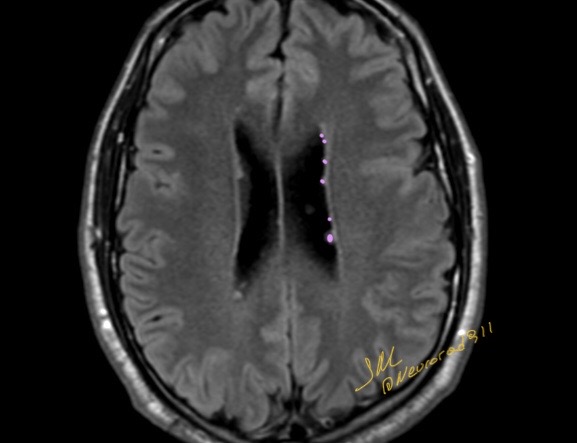
Ring-shaped lateral ventricular nodules (RSLVNs) were first described in 2009 by Shimono et al as incidental findings on brain magnetic resonance imaging examinations. They are commonly considered as benign asymptomatic lesions, with a reported prevalence of 0.45% in routine clinical practice brain MRI . Nevertheless, the exact nature of RSLVNs has not yet been fully clarified due to the lack of histopathologic confirmation, with different proposed hypotheses ranging from neuroglial cyst to a variant of subependymoma
Epithelioid angiosarcoma is a rare and highly aggressive endothelial cell malignant tumor with a high mortality rate. Although they often arise in sun-exposed skin (60% of the cases) and deep soft tissues such as the head and neck, they have been reported in other sites such as the breast, thyroid, kidney, bone, adrenal gland, vagina, testis, liver, and spleen . Angiosarcoma is a tumor with a high rate of recurrence and metastasis.
Radiographically, the findings of EHE are not specific; it can appear as an osteolytic lesion, and smaller lesions are usually well-defined, and larger lesions are ill-defined and permeative. The soap bubble appearance with expansion of bone has been described. It can present as solitary lesion in 60% of the cases or multifocal disease in 40% of the cases.
MRI findings of EHE are nonspecific, they include decrease in signal intensity on T1-weighted images, and isointense to slightly increase in signal intensity on T2-weighted images .
the differential diagnosis would include: metastatic disease, lymphoma, and myeloma. In young patients with multifocal disease the differential diagnosis includes brown tumor, Langerhans cell histiocytosis, and fibrous dysplasia. The differential diagnosis for solitary lesions includes fibrous dysplasia or sarcomas such as Ewing’s sarcoma, osteosarcoma, and fibrosarcoma .
Bertolotti syndrome, the association between an LSTV and low back pain, is controversial and has been both supported and disputed since Bertolotti first described it in 1917.
Clinical diagnosis of exclusion, given prevalence of LSTV.
Although not initially described, the low back pain of this syndrome is currently thought to be of varying etiologies, subsequently arising from different locations:
1) disk, spinal canal, and posterior element pathology at the level above a transition
2) degeneration of the anomalous articulation between an LSTV and the sacrum
3) facet joint arthrosis contralateral to a unilateral fused or articulating LSTV
4) extraforaminal stenosis secondary to the presence of a broadened transverse process
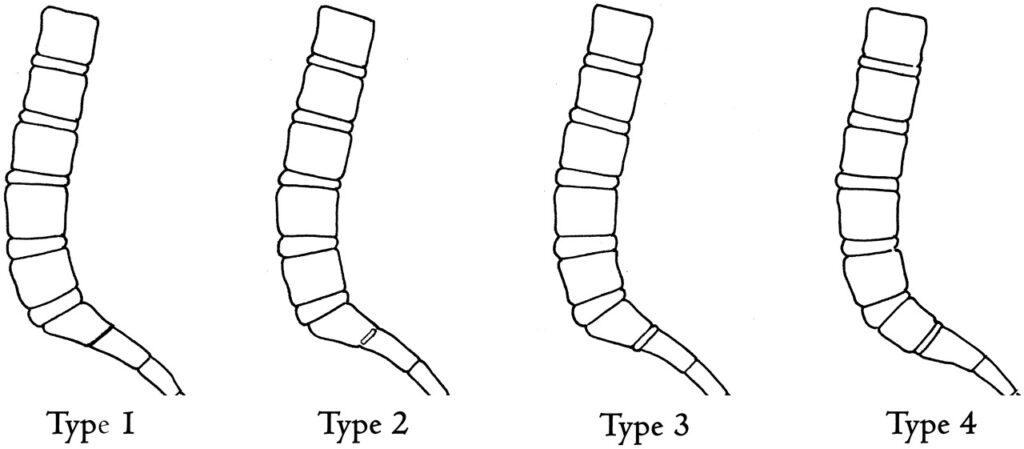
In most of the literature that supports Bertolotti syndrome, the implicated transitional segments are Castellvi types II-IV. Castellvi states that type I LSTVs are of no clinical significance and are a “forme fruste” and therefore have no relation to what was initially described as Bertolotti syndrome.
Illustration demonstrating the Castellvi classification of LSTVs.Illustration depicting the O’Driscoll classification system of S1–2 disk morphology.
Allergic fungal sinusitis is the most common form of fungal sinusitis. It is particularly common in warm, humid climates. The overall prevalence of allergic fungal sinusitis is estimated at 5%–10% of all patients with chronic hypertrophic sinus disease going to surgery.
The underlying cause is thought to be a hypersensitivity reaction to certain inhaled fungal organisms resulting in a chronic noninfectious, inflammatory process, similar to that seen in allergic bronchopulmonary aspergillosis of the lung. Although the exact pathophysiology is not yet clear, immunologically, immunoglobulin E–mediated type I immediate hypersensitivity and type III delayed hypersensitivity are thought to be involved.
Common implicated fungi are the dematiaceous (pigmented) fungi—Bipolaris, Curvularia, Alternaria—and the hyaline molds such as Aspergillus and Fusarium. Allergic fungal sinusitis is characterized by the presence within the affected sinuses of “allergic mucin”—inspissated mucus that is yellow-green, white-tan, gray, brown, or black with the consistency of peanut butter.
Allergic fungal sinusitis tends to be a disease of younger individuals, usually in their third decade. Typically, afflicted individuals are immunocompetent. There is a frequent associated history of atopy including allergic rhinitis and asthma. Patients usually experience chronic headaches, nasal congestion, and chronic sinusitis for several years. There is often a history of sinus surgery.
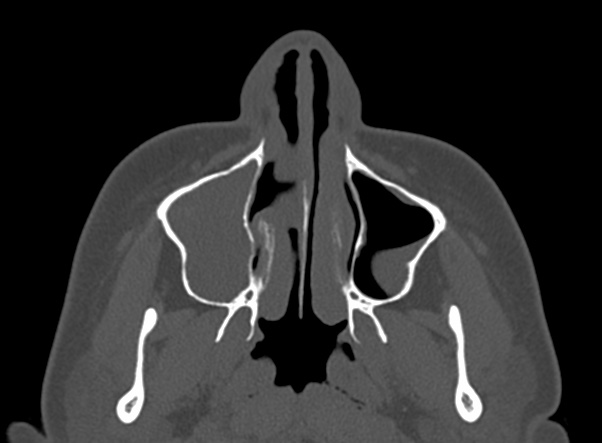
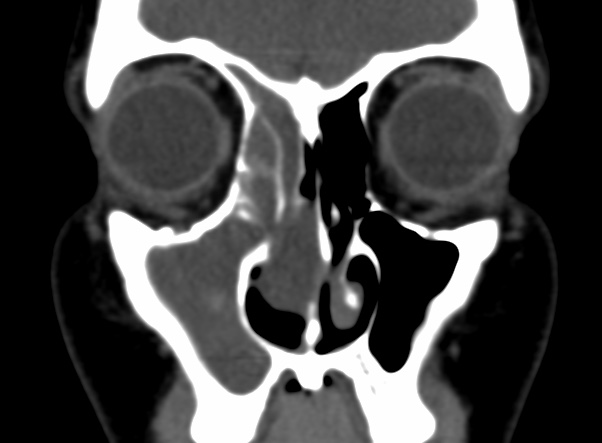
There is usually involvement of multiple sinuses if not pansinusitis and rhinitis. Disease tends to be bilateral, and there is a frequent nasal component. The majority of the sinuses show near-complete opacification and are expanded. Expansion, remodeling, or thinning of involved sinus walls is common in allergic fungal sinusitis (AFS) and is thought to be caused by the expansile nature of the accumulating mucin. Areas of high attenuation are found within the expanded paranasal sinuses in all patients. Similar radiographic findings can be caused by rare osteoid/chondroid matrix-producing sinonasal sarcomas or meningiomas.
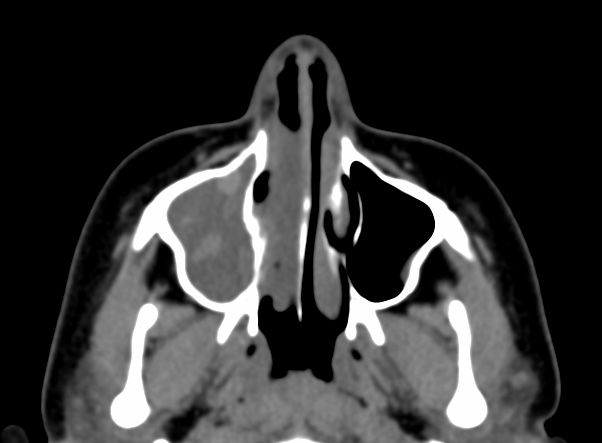
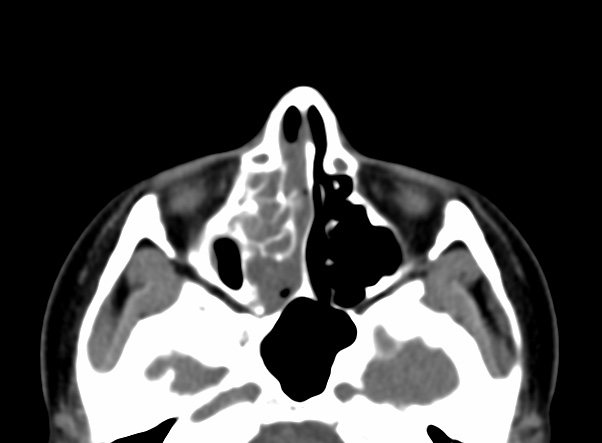
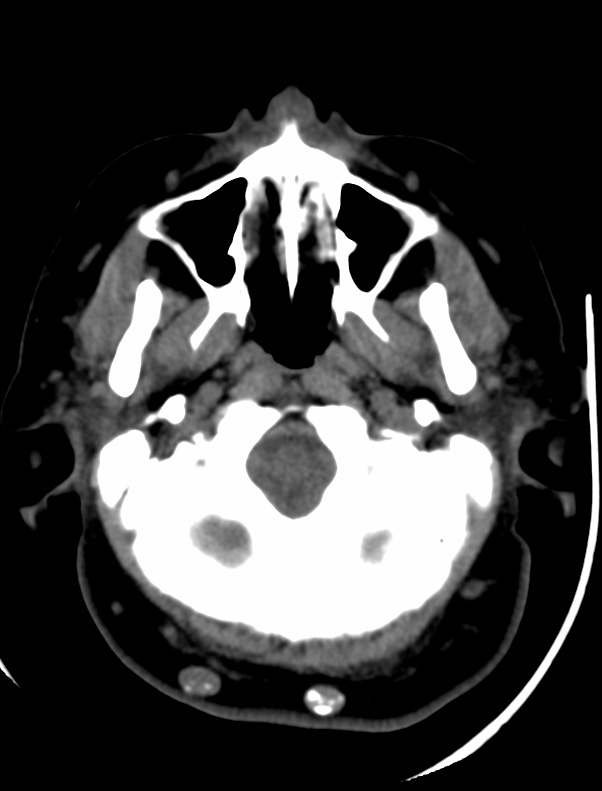
Noncontrast CT demonstrates hyperattenuating allergic mucin within the lumen of the paranasal sinus.
Bony erosion of the sinus walls and extension into adjacent cavities have been mentioned in many reports, usually focusing on intracranial extension, as depicted in the 1st image above.In most series, a rate of approximately 20% bony erosion with extension into surrounding vital cavities is reported.
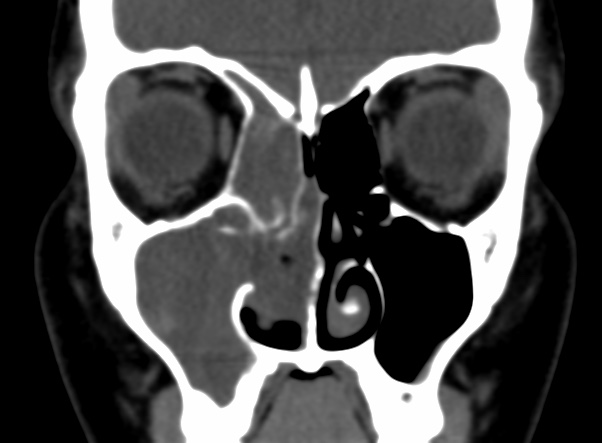
The ethmoid sinus was the most commonly involved sinus, while the adjacent lamina papyracea was the most common bone to exhibit demineralization, as depicted in the image below. Extension of allergic fungal sinusitis (AFS) beyond the confines of the paranasal sinuses most commonly occurred into the orbit, followed by the anterior, middle, and posterior cranial fossae, respectively
Although low signal intensity of the sinus contents has been described on T1-weighted images, we have frequently observed high signal intensity or mixed low, intermediate, and high signal intensity on T1-weighted images in these patients. There is characteristic low signal intensity or signal void on T2-weighted images. The T2 signal void is attributed to a high concentration of various metals such as iron, magnesium, and manganese concentrated by the fungal organisms. The T2 signal void is also attributed to a high protein and low free-water content of the allergic mucin.
The inflamed mucosal lining is relatively hypointense on T1-weighted images and hyperintense on T2-weighted images and demonstrates enhancement after intravenous administration of gadolinium contrast material.
There is no enhancement in the center or in majority of the sinus contents, which distinguishes this condition from neoplastic entities.
Although the condition is not considered invasive, if left untreated, the involved sinuses expand and there is smooth bone erosion with subsequent intracranial or intraorbital extension and resulting cranial or orbital symptoms. Intracranial extension is usually limited by the dura to the extradural space.
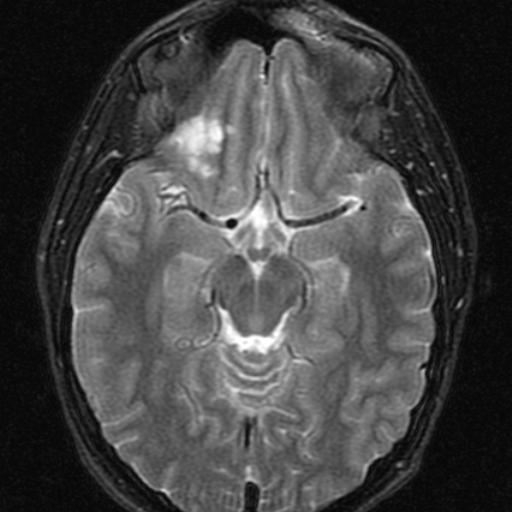
Dysembryoplastic neuroepithelial tumor is a benign tumor of neuroepithelial origin arising from the cortical or deep gray matter.These tumors virtually always manifest in patients with medically refractory partial seizures. The vast majority of patients are younger than 20 years, and males are more commonly affected. The temporal lobe is the most common site (62%), followed by the frontal lobe (31%). Although the vast majority of dysembryoplastic neuroepithelial tumors are confined to the cortical gray matter, they may also arise within the caudate nucleus, cerebellum, or pons.
he imaging appearance of dysembryoplastic neuroepithelial tumor is similar to those of other low-grade glial tumors, and in some cases it may be impossible to distinguish this tumor from diffuse astrocytoma, ganglioglioma, oligodendroglioma, or other low-grade neoplasms.
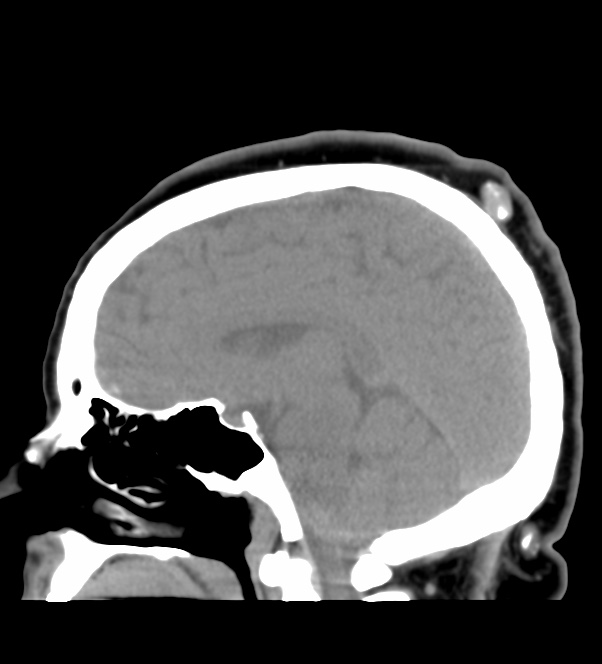
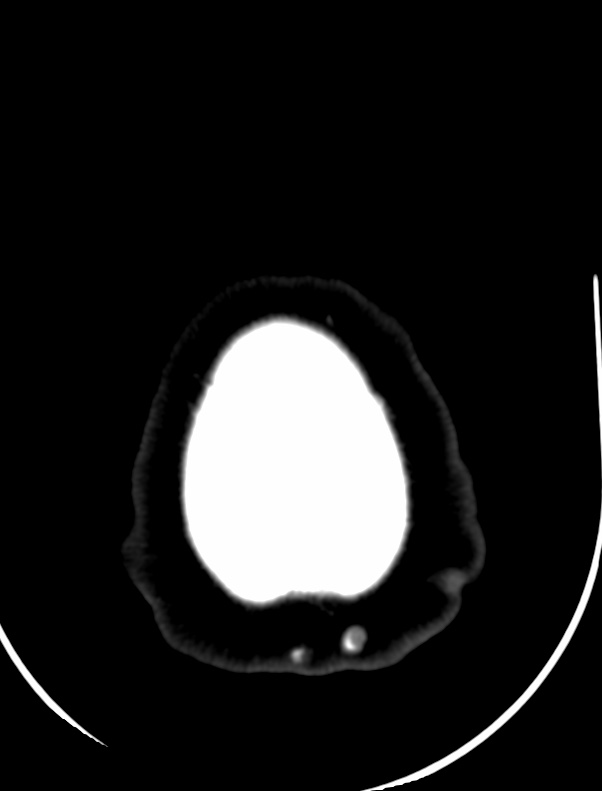
CT, the tumor manifests as a hypoattenuating mass that may occasionally have areas of calcification. Remodeling of the adjacent inner table of the skull may also be seen.
At MR imaging, dysembryoplastic neuroepithelial tumors most commonly manifest as cortical masses that are hypointense on T1-weighted images and hyperintense on T2-weighted images without surrounding vasogenic edema. ome lesions may appear as an enlarged gyrus, producing a soap bubble appearance at the cortical margin.
<30% of dysembryoplastic neuroepithelial tumors enhance following contrast.
Focal cortical dysplasia is commonly seen in association with DNETs, and unless a component can be identified clearly separate from tumor cells, then it does not warrant a concurrent separate diagnosis. If, however, such a separate component is present, then it represents Blumcke classification IIIb focal cortical dysplasia
Importantly, DNETs are negative for IDH mutations, TP53 mutations, and do not demonstrate 1p19q co-deletion 8. These features are helpful in distinguishing DNETs from low-grade astrocytomas (usually IDH mutated) and oligodendrogliomas (IDH mutated and 1p19q co-deleted).
Gaillard, F. WHO classification of CNS tumors. Reference article, Radiopaedia.org. (accessed on 20 May 2022) https://doi.org/10.53347/rID-2277DOI:https://doi.org/10.53347/rID-2277
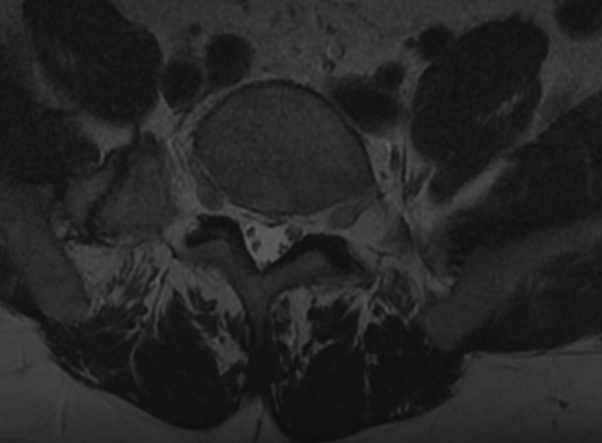
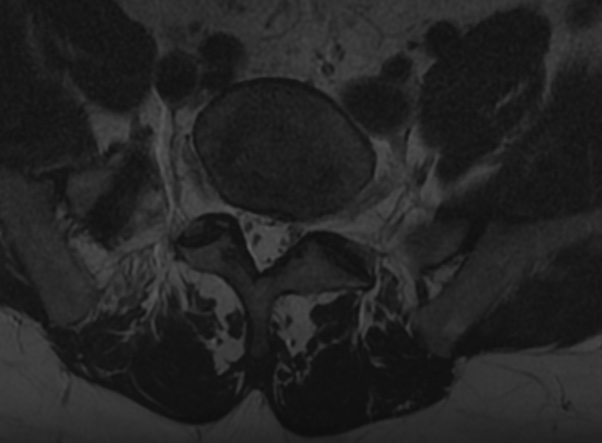
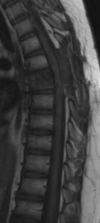
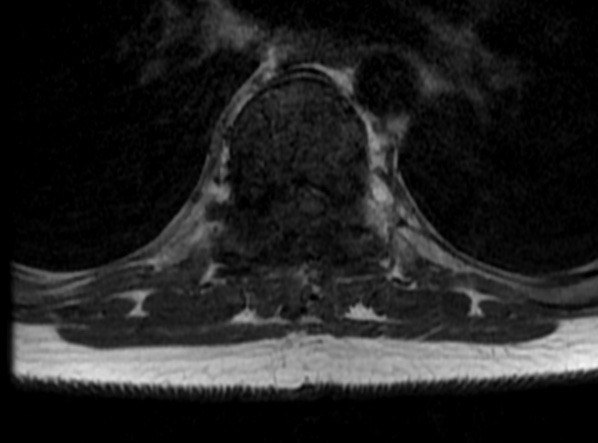
Vertebral haemangiomas are common vascular lesions affecting 11% of the population according to autopsy series. These lesions are usually asymptomatic and are discovered as incidental findings on multiple imaging modalities. Nevertheless, in some instances, these lesions can behave aggressively and cause pain or neurological deficit secondary to expansion of the vertebral body or paravertebral or epidural soft-tissue extension with spinal cord/nerve root compression.
Histologically, haemangiomas are predominantly composed of vascular lined spaces and non-vascular components that may include adipose tissue, smooth muscle, fibrous tissue, bone, haemosiderin and thrombus.
There are two histological subtypes of haemangioma: the cavernous type which is the most common subtype and is characterized by large sinusoidal spaces, and the capillary type which demonstrates smaller vascular channels.
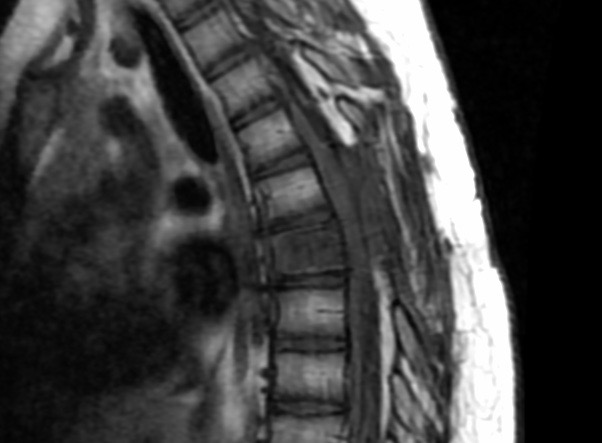
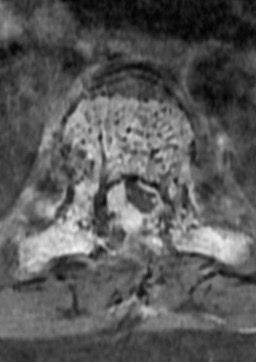
Vertebral haemangiomas classically have a coarse, vertical, trabecular pattern on radiographs which are seen on axial CT scan as punctate areas of sclerosis on axial imaging called “polka-dot” appearance or “jail-bar”, or “corduroy-cloth appearance” on sagittal or coronal reconstructions.
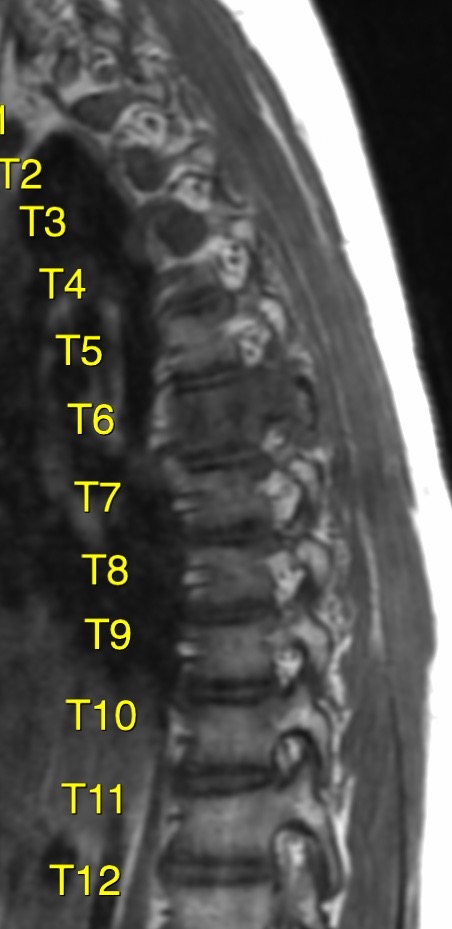
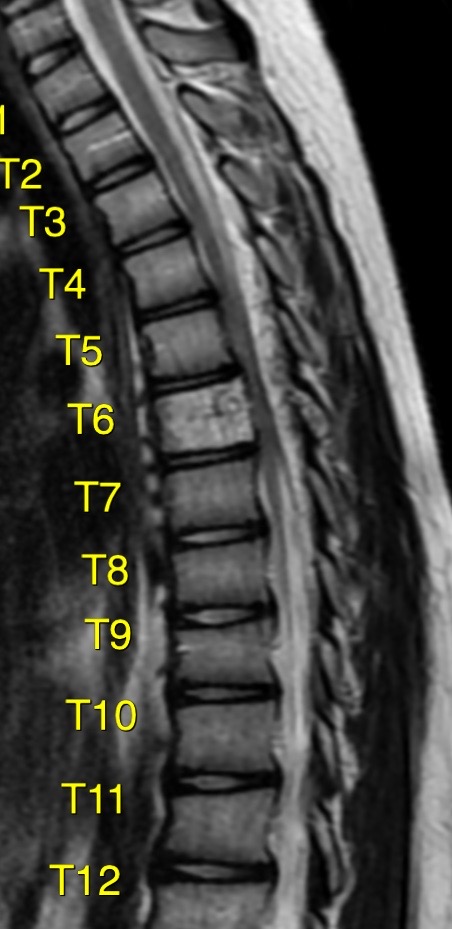
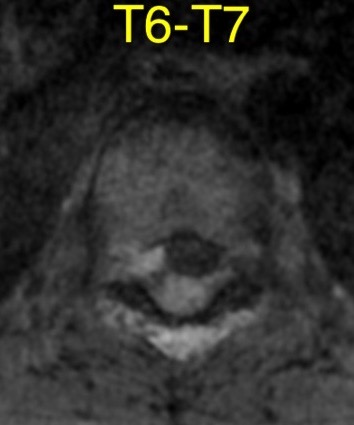
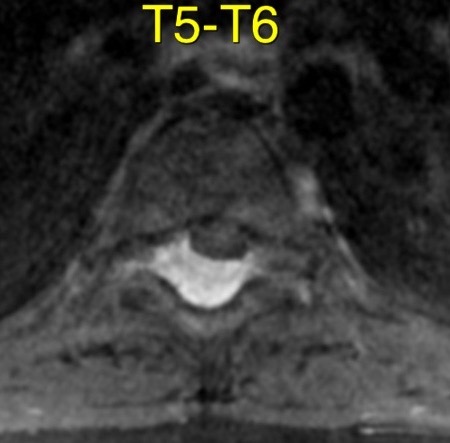
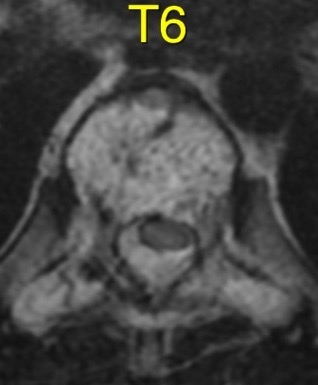
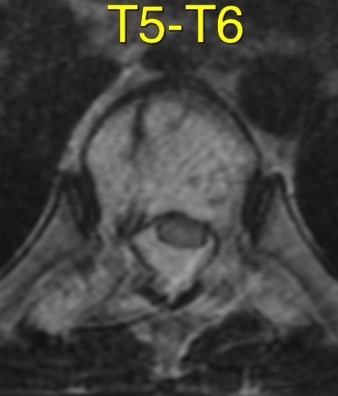
On MRI imaging, the signal intensity (SI) of typical asymptomatic haemangiomas is usually hyperintense on both T1 and T2 weighted sequences; however, aggressive haemangiomas have been shown to have low T2 SI related to paucity of adipose tissue.
The presence of adipose tissue in haemangiomas therefore has been suggested as a predictor of benign nature in some studies.
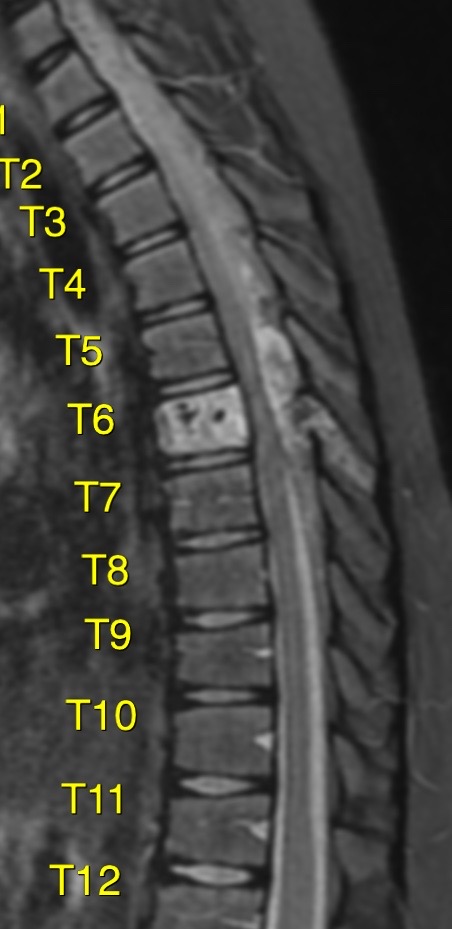
Laredo et al investigated the appearance of the stroma between the osseous trabeculae on vertebral haemangiomas and demonstrated absence of fat attenuation on CT in aggressive haemangiomas, in comparison to asymptomatic haemangiomas. In their study, aggressive haemangiomas showed numerous packed, thin-walled vascular cavities with absence of fatty replacement on histopathological evaluation. Ross et al and Pastushyn et al also demonstrated that the paravertebral extraosseous component of aggressive haemangiomas is hypointense on T1. In the study by Ross et al, histopathological evaluation of the extraosseous portion of the tumour showed a preponderance of angiomatous tumour vessels and fibrous tissue, with little adipose tissue. Although a few of the previous studies showed hyperintensity on STIR sequence in their published figures of aggressive haemangioma.
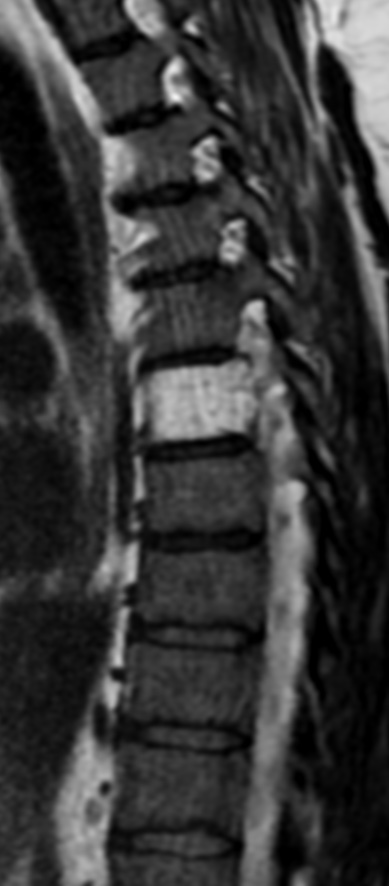
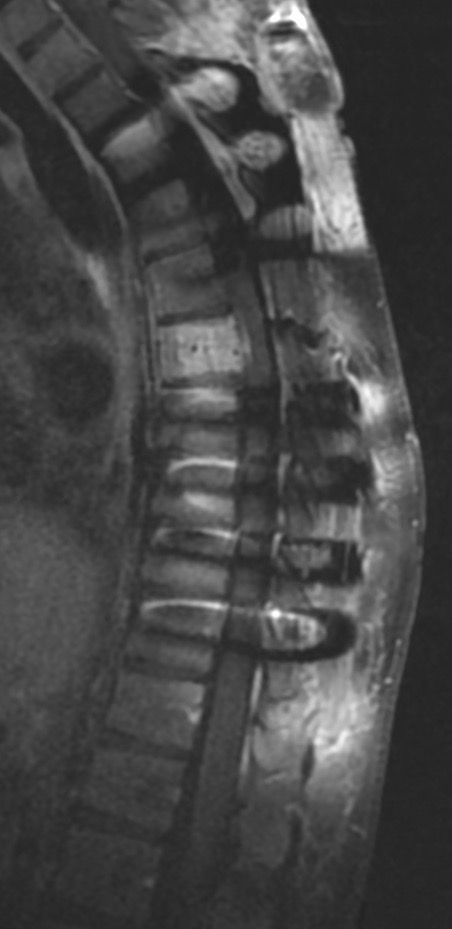
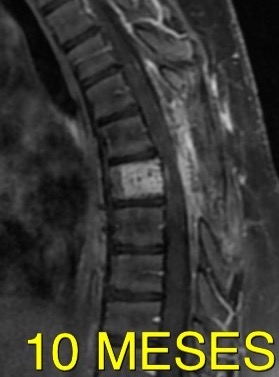
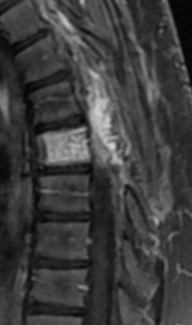
A 13-year-old boy presented with only 3 weeks duration of progressive ataxia,intense back pain, hypoaesthesia and hyperreflexia of both lower limbs.
Vertebral haemangiomas are the most common tumours of the spine, with an estimated incidence of 10–12% of the population and may occur in the posterior elements, vertebral body or all three columns. Despite its high incidence, only 0.9–1.2% of these are symptomatic in adults.
This figure is much lower in the paediatric population, with a total of 5 cases reported in the literature up to 2011.
Unlike the adult population, the natural course of symptomatic childhood vertebral haemangiomas is highly variable. the reports of vertebral haemangiomas in the paediatric age group have suggested that they tend to behave more aggressively compared to those in adults, whom are known to have slow progressive neurological deficits of an insidious nature.
The hyperintense T2 signal is due to the fatty component of the tumour and this allows better differentiation from other highly cellular neoplasms and lymphomas.
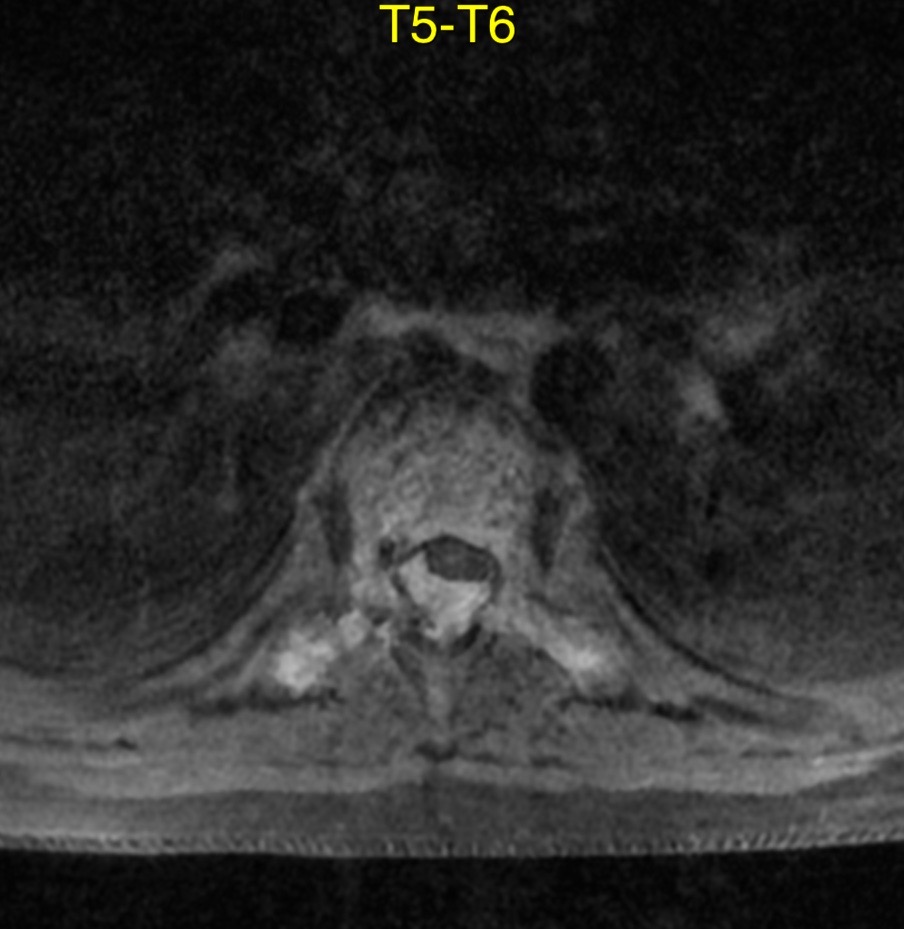
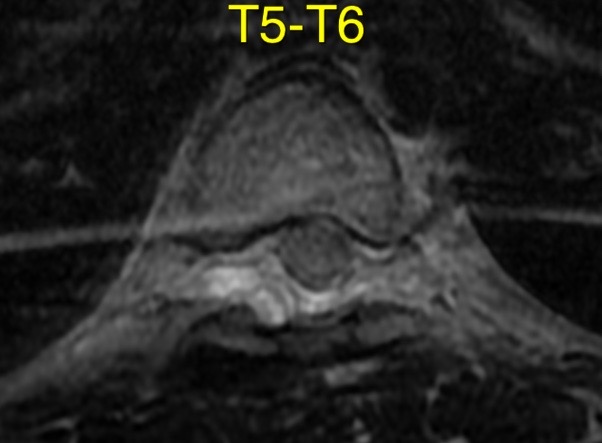
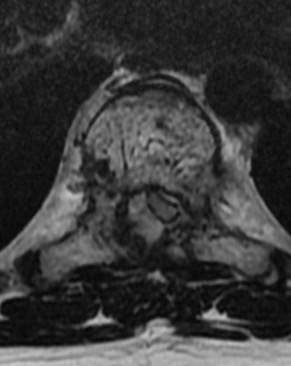
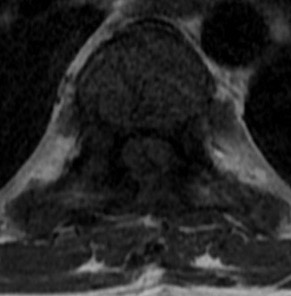
T1T2STIRCONTRAST FATSATCONTRAST FAT SAT AND AXIAL T2PRESURG- SURG-PPOSTSURG
Treatment: Surgery in cases of rapid or progressive neurologic symptoms: compressive myelopathy or radiculopathy Radiotherapy for patients with slow progressive neurologic deficits Recently, there has been increasing interest in the management of symptomatic lesions using vertebroplasty, transarterial embolization, and direct intralesional ethanol injection
presurg6 month after surgery10 month later -worstre operated-control1 estudio prequirurg. contrasteaxial t1 Gd-1 estudios1 estudiopost quirurg 6 mese seg estestudio 2doestudio 2doestudio 3ro-peor mielopatia
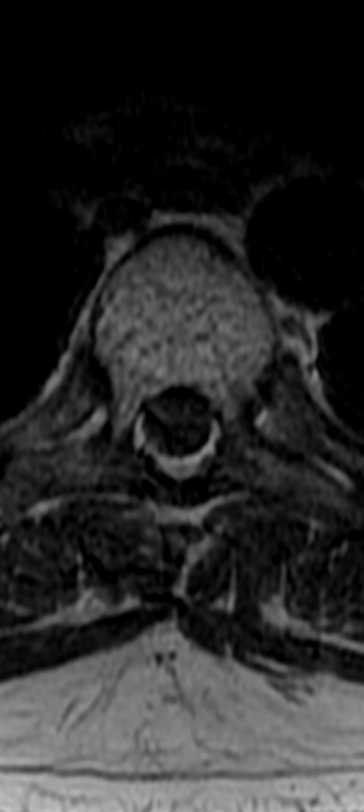
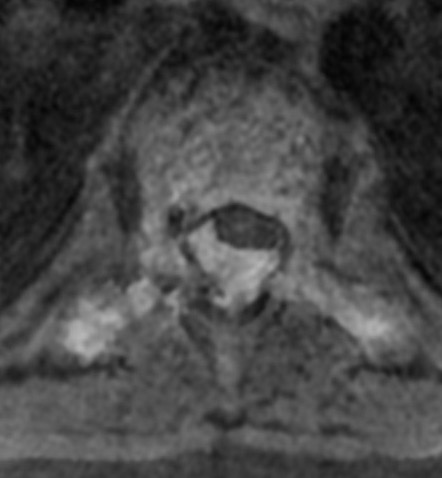
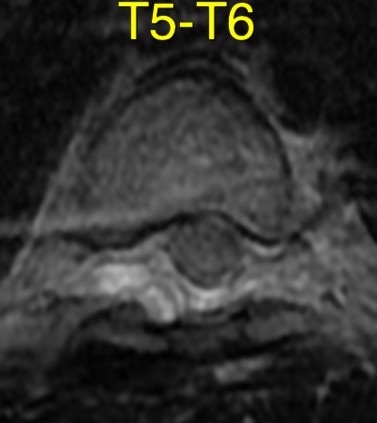
Hemangiomas can be classified as typical, atypical and aggressive (compressive). These are benign tumors composed of capillary-sized to cavernous blood vessels. The term aggressive refers to the presence of radiologic features such as extension beyond the vertebral body, destruction of the cortex, and invasion of the epidural and paravertebral spaces. Aggressive hemangioma can occur at any age, with peak prevalence in young adults, and is localized preferentially in the thoracic spine.
Neurologic symptoms due to compression of the spinal cord, nerve roots, or both, leading to myelopathy and/or radiculopathy Clinical worsening and growth during pregnancy is a well known phenomenon. The main explanation is vena cava compression and re-routing of blood to the paravertebral, epidural, and acygous venous system.
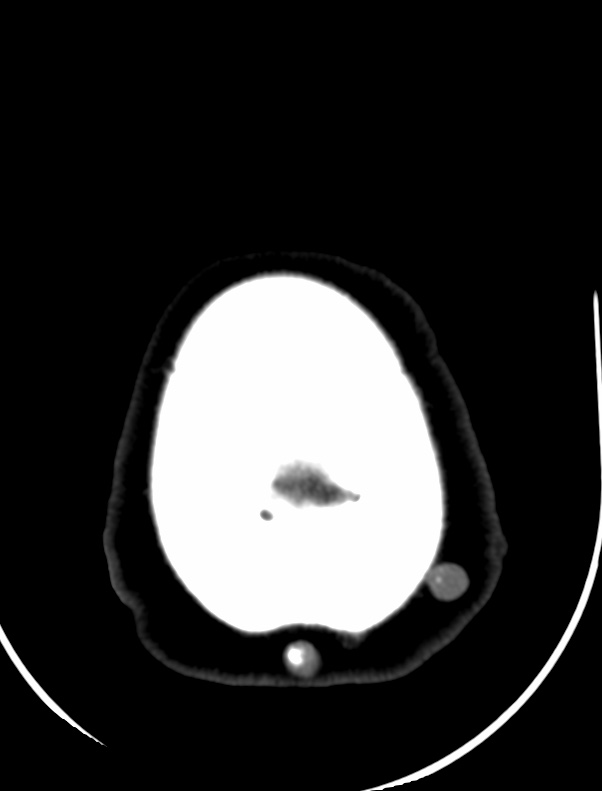
CT scan reveals hypodense expansile vertebral body mass, with soft tissue extension and spinal cord/nerve root compression. Typical «polka-dot» and «corduroy» signs can guide the correct diagnosis.
MRI shows a T1 hypointense, high-T2 lesion with variable contrast enhancement. Aggressive hemangiomas are difficult to diagnose by MRI because findings overlap with those of metastatic disease and focal bone marrow infiltration.
Differential Diagnosis: Metastases: Findings that favor an aggressive hemangioma over a metastasis are maintained vertebral body height, a sharp margin with normal marrow, intact cortex adjacent to a paraspinal mass, enlarged paraespinal vessels, and the «polka dot» sign on axial images. Solitary bone plasmocytoma: Classically, plasmocytomas can have a «mini brain» appearance on axial CT and MR imaging (thickened cortical struts resemble the sulci seen in the brain) or, less typically, multicystic «soap bubble» appearance. Lymphoma: The epidural component of a vertebral lymphoma appears less hyperintense on T2W compared with the hypervascular component of aggressive hemangioma. Epitheloid hemangioendothelioma: Lytic pattern of bone destruction with mixed signal intensity on T1- and T2-weighted MRI due to the absence of fat and the presence of inflammatory infiltrate
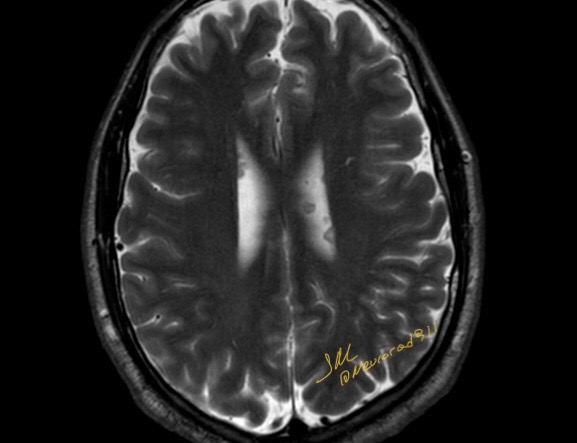
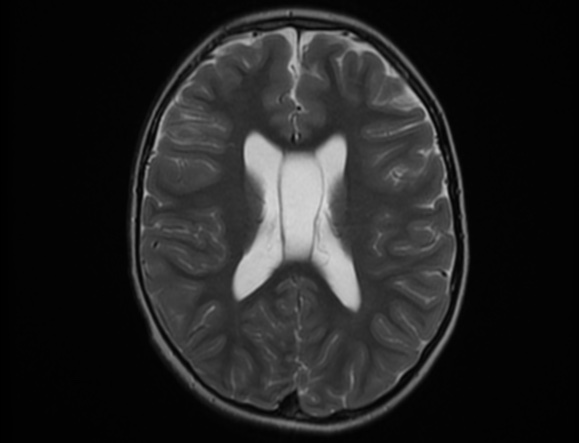
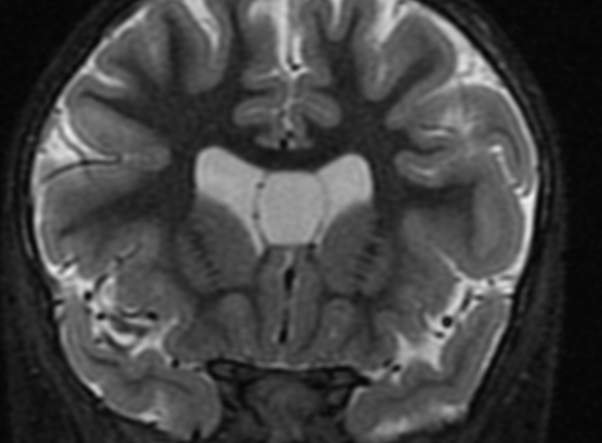
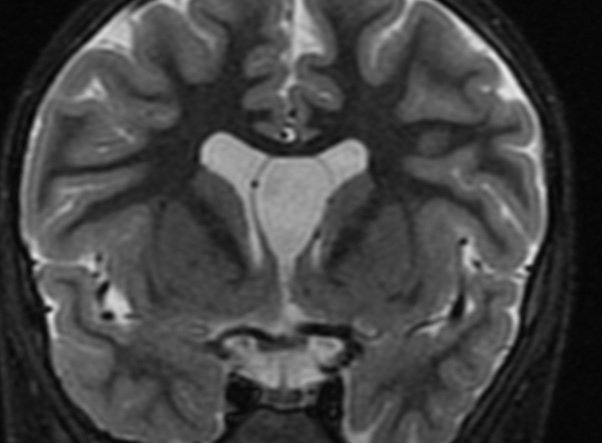
The septum pellucidum is a structure that is marginated by the corpus callosum and body of the fornix. It is composed of white matter leaves along the medial walls of the lateral ventricles and is lined by ependyma along its ventricular surfaces . The entire space between the leaves of the septi pellucidi is the cavum septi pellucidi et vergae, with the space anterior to either the foramina of Monro or an arbitrary vertical plane formed by the forniceal columns being the CSP and the space posterior being the cavum vergae.
When the two leaves fail to fuse and form the septum pellucidum, a number of postnatal anatomic variants can result including the CSP, cavum vergae, and cavum veli interpositi. The CSP and the cavum vergae usually freely communicate with one another. Usually a cavum vergae is seen in association with a CSP, although it can also occasionally be seen in isolation . In general, persistence of the CSP in postnatal life is considered a normal variant.
The leaves of the septi pellucidi begin to close at approximately 6 months’ gestational age from back to front. Nearly all term infants have closure of the cavum vergae and the majority of infants 3–6 months old have closure of the cavum septi as well . The cavum sometimes persists into adulthood as a normal variant, typically small, measuring less than 4 mm in transverse diameter, in healthy individuals . The terminology can be confusing. In general, when the two leaves are separated, this may be referred to as the “cavum septi pellucidi” or “CSP”; when the leaves are fused to form a single structure, it is referred to as the “septum pellucidum”
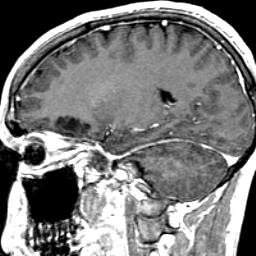
The usual clinical presentation of PTT is that of a long-standing, subcutaneous, cystic nodule that slowly progresses to a large, nodular mass, often following a history of trauma or inflammation. The tumor preferentially arises in areas of dense hair follicle concentrations, and about 90% of cases occur on the scalp, with the residual 10% occurring mainly on the back. Other, less common locations include the vulva, nose, mons pubis, buttock, wrist, chest, and elbow.
Women are affected in more than 80% of cases, and the average age of patients is 65 years . The presentation is nearly always that of a single lesion, but, rarely, multiple lesions are seen.
Areas of necrosis, calcification, and hyalinization may be seen. The stroma is usually fibrous and shows a variable inflammatory reaction, including foreign body giant cells.
Although PTT is generally considered biologically benign, even though histologically indistinguishable from squamous cell carcinoma in some cases, malignant PTT has been reported. Saida et al suggested three stages in the oncologic development of a malignant PTT: the adenomatous stage of the trichilemmal cyst, the epitheliomatous stage of the PTT, and the carcinomatous stage of the malignant PTT. A rare occurrence of PTT with spindle cell carcinoma has also been reported .
Reference:
American Journal of Neuroradiology January 2001, 22 (1) 180-183;
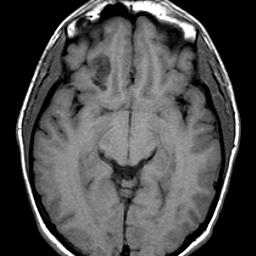
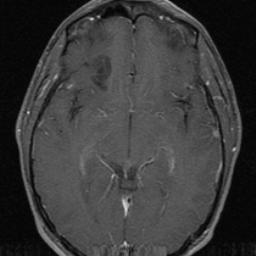
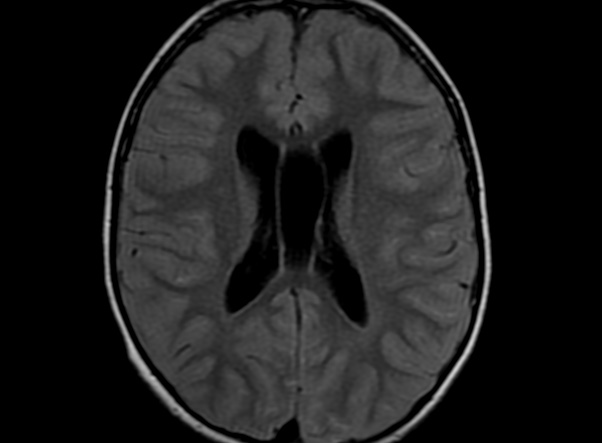
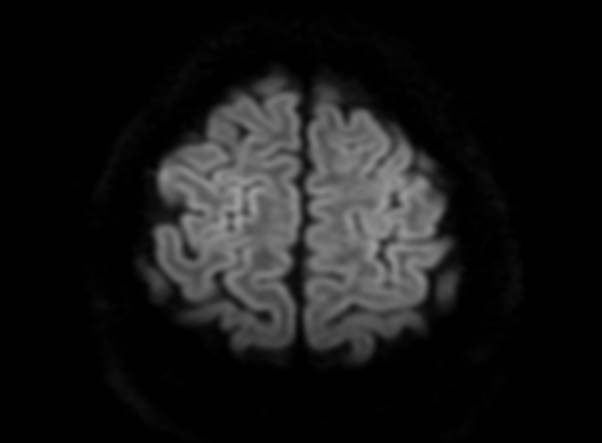
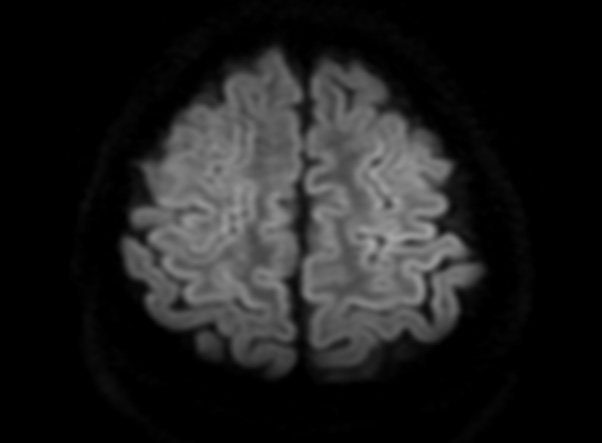
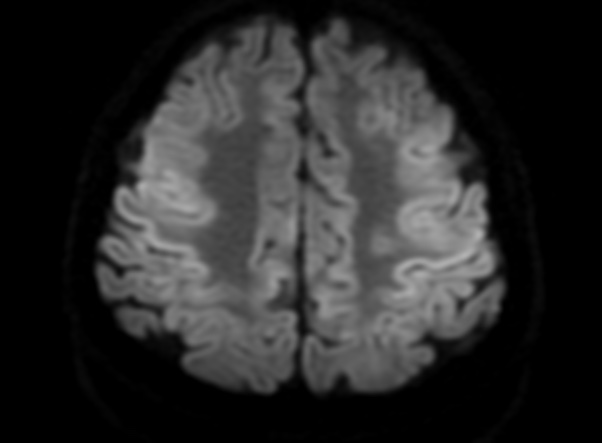
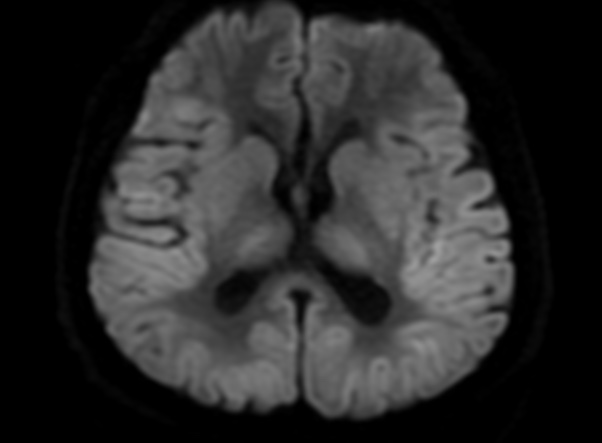
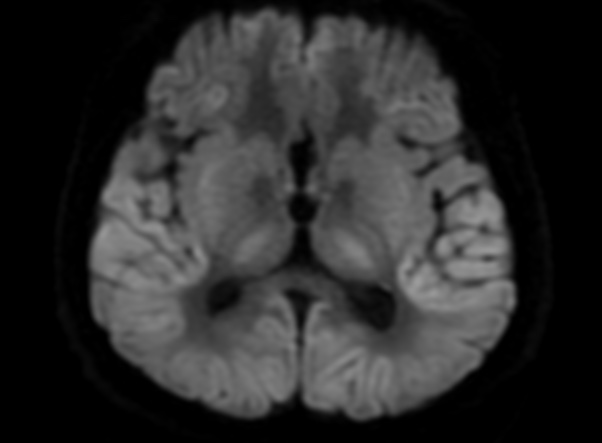
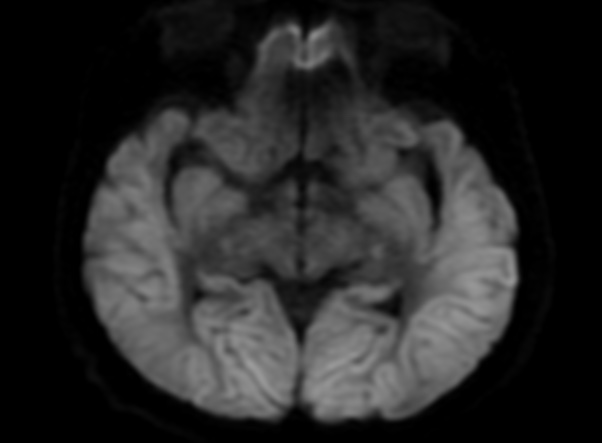
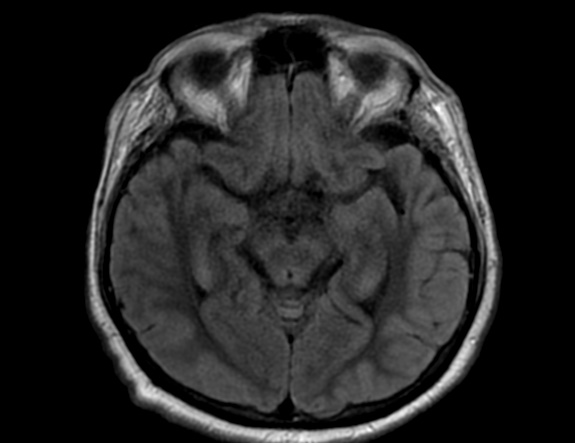
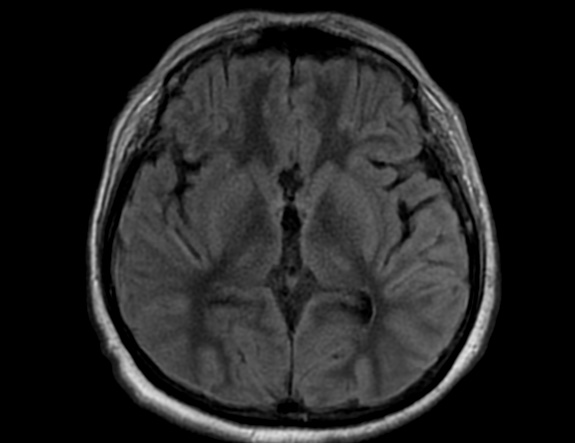
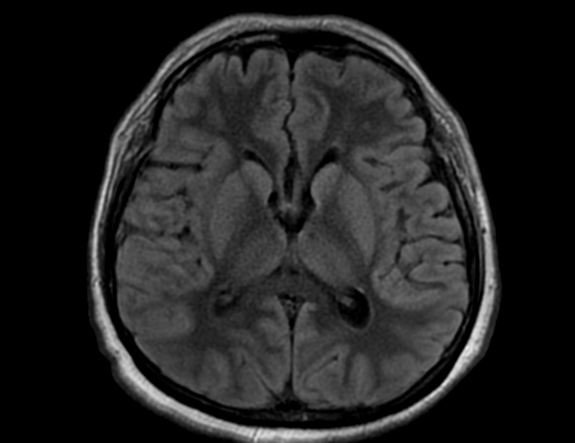
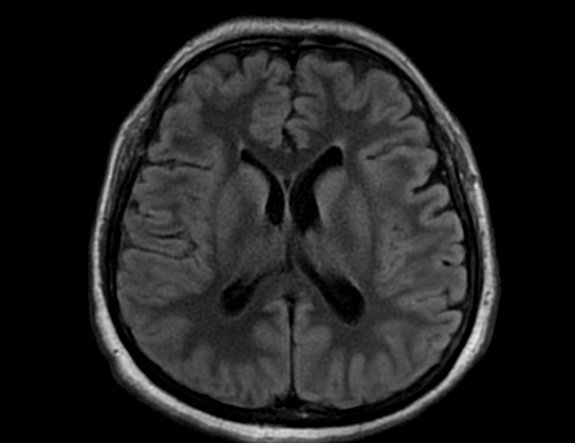
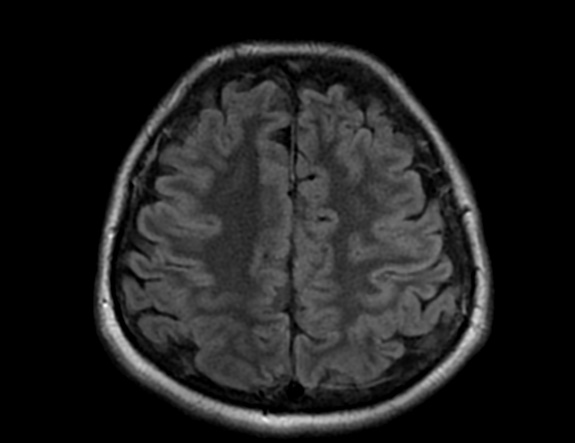
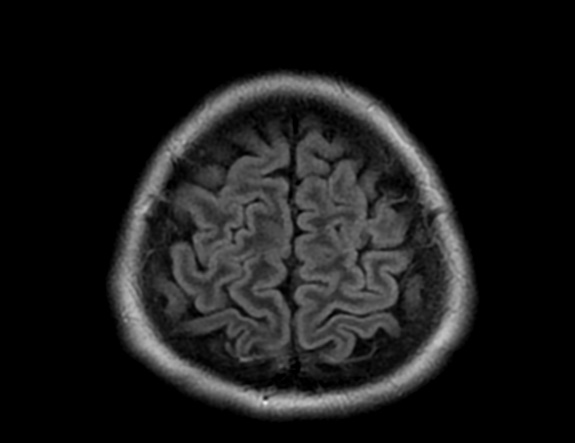
FLAIR image show symmetric hyperintense lesions in the parietal cortices bilaterally.
Diabetic ketoacidosis with prolonged hyperglycemia may cause subtle FLAIR and diffusion abnormalities in the cortex associated with elevations in glucose, myoinositol, taurine, and ketones in MR spectroscopy.
Diabetes mellitus type 1 (DM1) is one of the most common chronic pediatric illnesses. Diabetic ketoacidosis (DKA) is serious complication in children with DM1 and has an increasing incidence. DKA is a state of severe insulin deficiency, either absolute or relative, resulting in hyperglycemia, ketonemia, acidemia, and systemic inflammation.
DKA is a rather common presentation or complication of pediatric DM1 patients and occurs in about 36% of diabetic children younger than 5 years of age and about 16% of teenagers older than 14 years. In the majority of pediatric patients, DKA has an excellent prognosis. In about 1% of the children DKA results in acute morphologic and functional brain changes that are associated with poor long-term neurocognitive outcome. Neuroimaging plays a key role in the early diagnosis of diabetic children with DKA and acute CNS involvement. Accordingly, it important that neuroradiologists are aware of the possible neuroimaging findings associated with DKA.
Cerebral edema is the most common neuroimaging finding associated with pediatric DKA and occurs in about 0.5%–1% of pediatric DKA.
Cerebral edema in DKA is associated with increased morbidity and mortality in up to 50% of affected children and occurs almost exclusively in pediatric patients. Children with more severe acidosis, hypocapnia, and dehydration have a higher risk of developing cerebral edema. The exact pathomechanism of cerebral edema in DKA, however, remains unclear and is most likely multifactorial. Possible pathomechanisms include (1) osmotic gradients drawing fluid into hypertonic astrocytes during intravenous therapy, (2) intracellular accumulation of sodium and water as a correction of intracellular acidosis due to the accumulation of lactate, free fatty acids, and ketone bodies, and (3) vasodilatation and reperfusion following cerebral vasoconstriction due to hypoocapnia.
On CT and MRI, cerebral edema in children with DKA is characterized by effacement of the sulci and basilar cisternal spaces (especially the suprasellar, quadrigeminal plate and ambient cisterns), compression and decreased size of the cerebral ventricles, and reduction of the gray-white matter differentiation.
Diffusion-weighted and diffusion-tensor imaging may further characterize cerebral edema and differentiate between vasogenic and cytotoxic edema. Increased ADC values representing vasogenic edema have been shown in the basal ganglia, thalamus, frontal white matter, and periaqueductal gray matter of children with DKA and cerebral edema. Increase in ADC values correlates with the degree of dehydration and hyperventilation at presentation, but not with factors related to initial osmolality or osmotic changes during treatment.These findings suggest that cerebral hypoperfusion may be a key role in the pathomechanism of cerebral edema in DKA. The role of cerebral hypoperfusion is supported by perfusion-weighted imaging studies showing shorter mean transit times and higher peak tracer concentrations, again suggesting vasogenic edema.
Severe cerebral edema may cause complications with high morbidity and mortality such as focal stroke and subfalcine or transtentorial herniation. Focal infarction secondary to cerebral edema may occur in up to 20% of children with DKA and typically involves the mesial basal ganglia, thalamus, periaqueductal gray matter, and dorsal pontine nuclei. Brain herniation is an uncommon complication of cerebral edema in DKA that typically occurs 6–13 hours after onset of symptoms and is clinically characterized by sudden deterioration of consciousness, absent brainstem responses, and eventual respiratory arrest. Compression of the major vessels of the circle of Willis due to downward herniation may play an additional significant factor in the occurrence of focal ischemic strokes.
Other possible neuroimaging findings in DKA include ischemic and hemorrhagic stroke, sinovenous thrombosis, and extrapontine myelinolysis. Ischemic stroke in DKA may occur independently from cerebral edema and be due to increased blood viscosity and thrombosis due to hyperosmolality, systemic inflammatory reaction, vascular endothelial injury, acidemia-induced red blood cell rigidity, and hyperglycemia-induced vasoconstriction. Hemorrhagic stroke is less common in acute DKA and may be secondary to sinovenous thrombosis.
In addition, hyperglycemia and acidosis could enhance endothelial damage with subsequent extravasation of red blood cells through the leaky vessels and increase the risk of hemorrhagic transformation of ischemic strokes.
Finally, extrapontine myelinolysis is a very rare complication. Extrapontine myelinolysis is characterized by T2-/FLAIR-hyperintense signal and restricted diffusion in the claustrum and putamen with inconsistent involvement of the hippocampi and subcortical white matter and may be associated with pontine myelinolysis. The exact pathomechanism of extrapontine myelinolysis in DKA is unknown, but is most likely related to electrolyte imbalance in the context of DKA and its rapid correction.