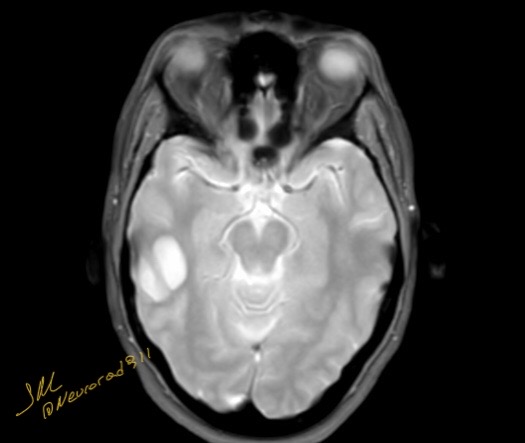
Neuroepithelial cysts, also known as glioependymal cysts, originate from the area surrounding the craniospinal axis (ie, orbital, intraspinal, perispinal, sacral, and pericranial). The cysts develop from ectopic ependymal cells.
Both MRI and CT play an essential role in establishing a diagnosis, although MRI is the preferred modality for identifying neuroepithelial cysts. The cyst has smooth, rounded borders and is composed of thin, unilocular walls that contain CSF-like fluid that is identifiable on CT or MRI. CT scans generate a cystic focus with unenhanced low-density fluid, and MRI shows a cystic-filled lesion with fluid that is hypointense on T1-weighted and hyperintense on T2-weighted images. Moreover, the contents of the cyst show no restriction in the diffusion-weighted sequence, which is comparable to CSF and no surrounding edema. The mass effect caused by these cysts is minimal, even in prominent lesions, indicating their marginal growth, especially in adults. There is no enhancement after contrast media injection
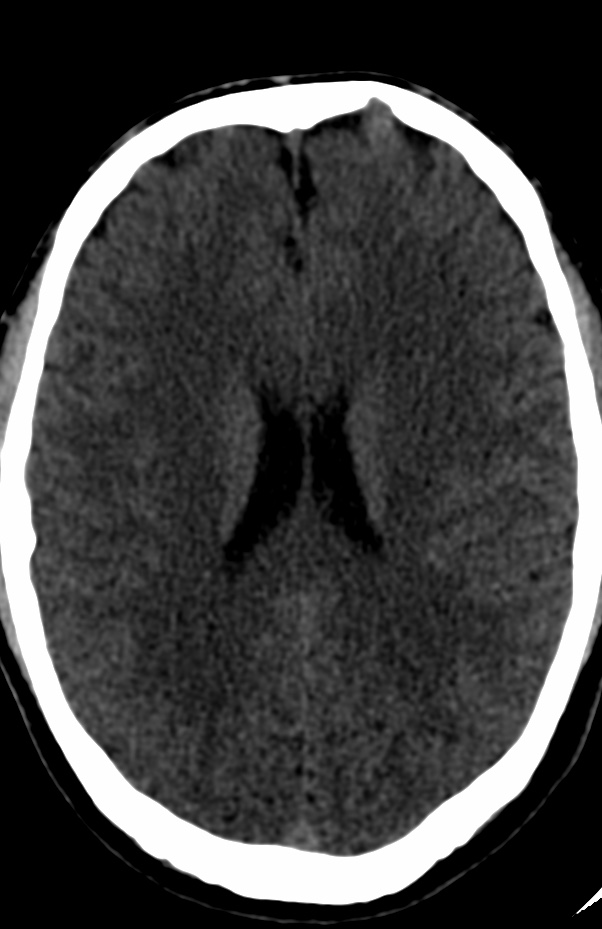
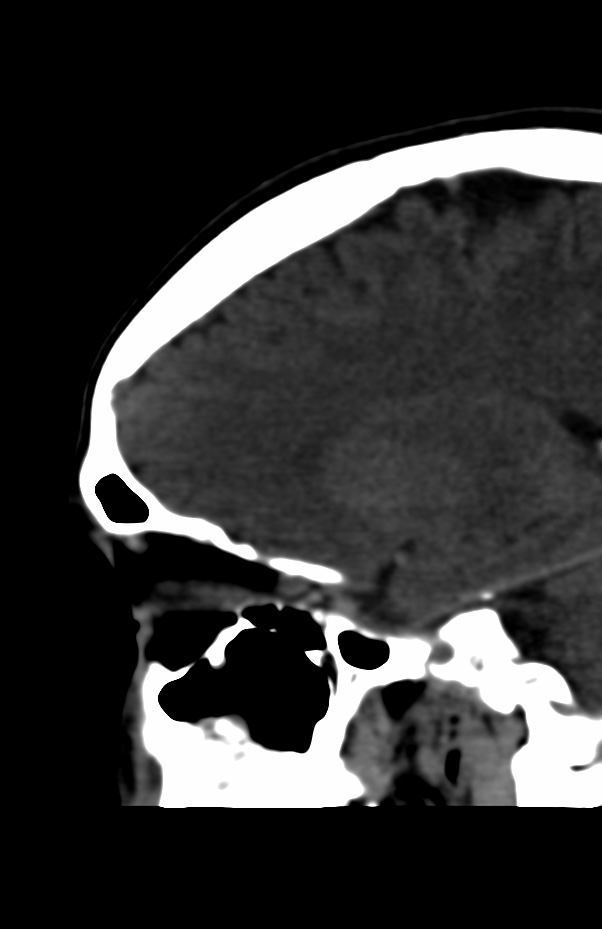
An incidental frontal encephalocele is an abnormality of the skull in which a sac-like structure containing brain tissue and cerebrospinal fluid (CSF) protrudes through a defect in the frontal region of the skull. An incidental encephalocele is one that is discovered by chance during imaging studies done for other reasons.
There is a rare association between frontal encephaloceles and epilepsy, where patients with encephaloceles may present with seizures. The exact mechanism of this association is not clear, but it is thought that the presence of brain tissue within the encephalocele sac may cause abnormal electrical activity that leads to seizures.
However, it is important to note that not all patients with an incidental frontal encephalocele will develop epilepsy or other neurological symptoms. In fact, many patients with incidental encephaloceles are asymptomatic and the encephalocele is discovered incidentally during imaging studies for other reasons.
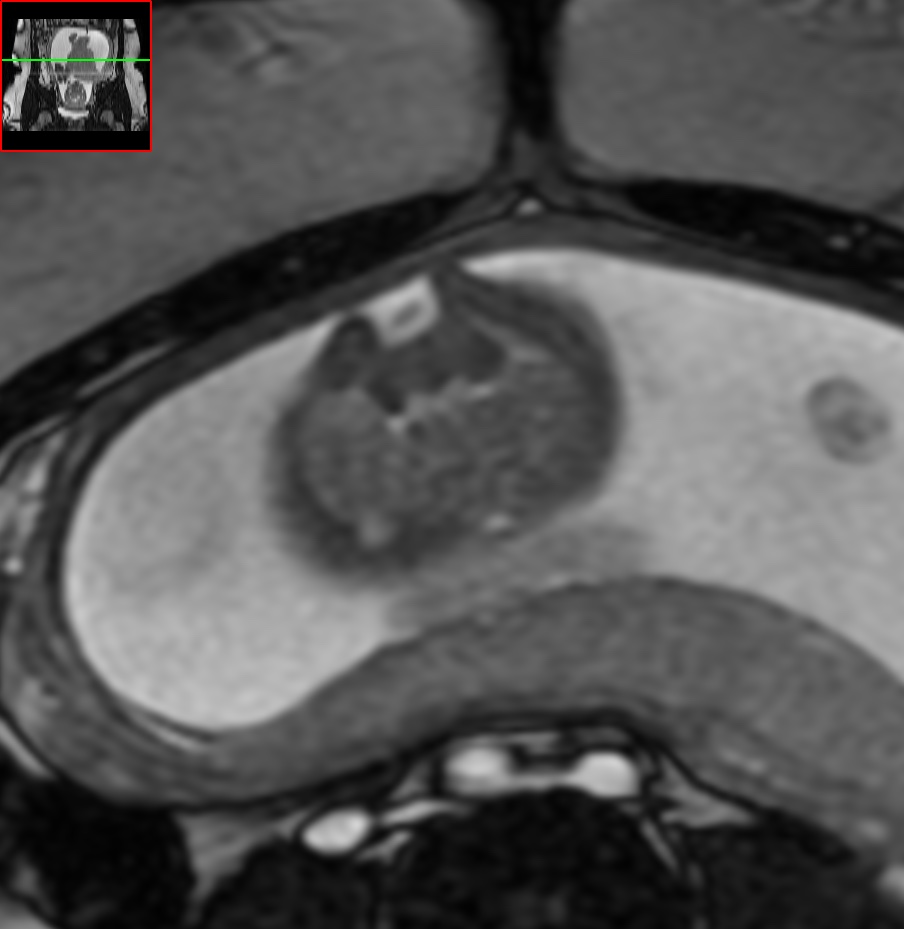
On MRI, a quadrigeminal plate lipoma appears as a mass with high signal intensity on T1-weighted images and low signal intensity on T2-weighted images. This is because the tumor is composed of fat, which has a high signal intensity on T1-weighted images and a low signal intensity on T2-weighted images. The tumor may also demonstrate a characteristic «Y» shape, which corresponds to the normal anatomic configuration of the quadrigeminal plate region.
In some cases, a quadrigeminal plate lipoma may be associated with hydrocephalus, which is the accumulation of cerebrospinal fluid in the brain. This can occur due to compression of the cerebral aqueduct, which is a narrow channel that connects the third and fourth ventricles in the brain. MRI can also be used to evaluate for the presence and extent of hydrocephalus, which appears as enlargement of the ventricles on T2-weighted images.
It is important to note that quadrigeminal plate lipomas are typically asymptomatic and do not require treatment. However, in some cases, they may be associated with hydrocephalus or other neurologic symptoms, which may require further evaluation and management.
Cochlear hydrops is a condition that affects the inner ear and can result in hearing loss, tinnitus, and vertigo. is a useful imaging modality for evaluating cochlear hydrops, particularly using a technique called delayed contrast-enhanced MRI.
Endolymphatic hydrops is further classified into two subtypes: type 1 and type 2. MRI is a useful imaging modality for evaluating endolymphatic hydrops, including type 1 hydrops.
On MRI, type 1 endolymphatic hydrops typically appears as a distention or dilation of the endolymphatic compartment of the inner ear. This can be seen as a dilation of the endolymphatic sac, which is the structure that regulates the volume and pressure of the endolymphatic fluid within the inner ear. Additionally, there may be enhancement of the endolymphatic sac, which is a result of the accumulation of contrast material within the dilated sac.
Other potential MRI findings in type 1 endolymphatic hydrops may include fluid-filled spaces in the cochlea or vestibule, which are structures within the inner ear that are responsible for hearing and balance, respectively. These fluid-filled spaces may be dilated or distended, and may show enhancement on post-contrast images.
It is important to note that MRI is not always necessary to diagnose endolymphatic hydrops, and other imaging modalities such as CT or electrocochleography may also be used. Additionally, the diagnosis of endolymphatic hydrops is often based on a combination of clinical symptoms and imaging findings.
In delayed contrast-enhanced MRI, contrast material is injected intravenously, and images are acquired after a delay of approximately 4 hours. This technique is useful for evaluating the degree of endolymphatic hydrops, which is the accumulation of excess fluid within the inner ear that is characteristic of cochlear hydrops.
On delayed contrast-enhanced MRI, the inner ear structures may demonstrate delayed enhancement, which corresponds to the presence of excess fluid within the endolymphatic spaces. This delayed enhancement can be seen in the cochlea, vestibule, and semicircular canals, and is a hallmark of cochlear hydrops.
In addition to delayed contrast-enhanced MRI, other imaging modalities such as CT and conventional MRI may also be used to evaluate cochlear hydrops. These imaging modalities can show the presence of fluid in the inner ear, and may also be used to identify potential causes of the condition, such as Meniere’s disease or autoimmune inner ear disease.
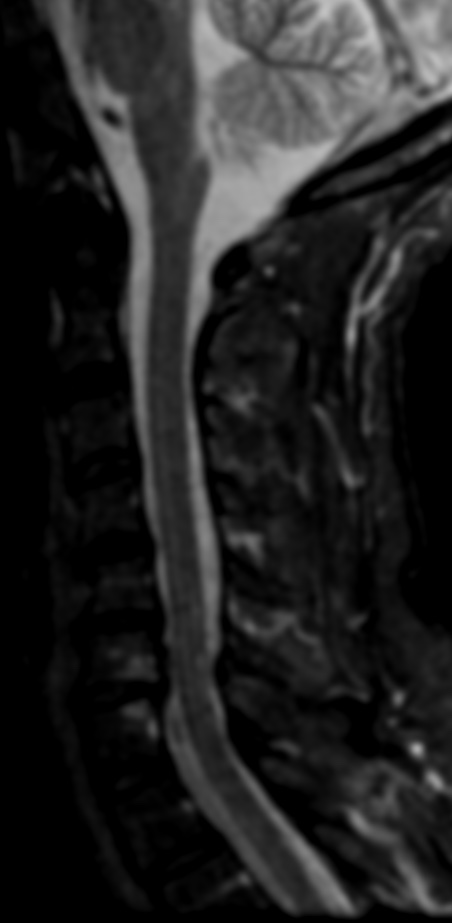
Posterior cervical myelopathy refers to a condition where there is compression of the spinal cord in the cervical spine, specifically in the posterior region of the spine. MRI is a useful imaging modality for evaluating cervical myelopathy, as it can show the extent and location of spinal cord compression.
On MRI, findings of posterior cervical myelopathy may include:
Narrowing of the spinal canal: The spinal canal may appear narrower than normal due to degenerative changes, herniated discs, or bone spurs. This narrowing can lead to compression of the spinal cord.
Signal changes in the spinal cord: Compression of the spinal cord can cause changes in the signal intensity of the spinal cord on MRI. These changes may be due to edema, myelomalacia, or gliosis .
Disc herniation: Herniated discs can compress the spinal cord and lead to symptoms of myelopathy. On MRI, a herniated disc can be visualized as a bulging or protruding disc material beyond the normal confines of the disc space.
Osteophytes or bone spurs: Osteophytes or bone spurs may form along the edges of vertebral bodies due to degenerative changes. These spurs can impinge on the spinal cord and cause compression.
Ligamentum flavum hypertrophy: The ligamentum flavum is a ligament that runs along the back of the spinal canal. It can become thickened or hypertrophied due to degenerative changes, which can lead to compression of the spinal cord.
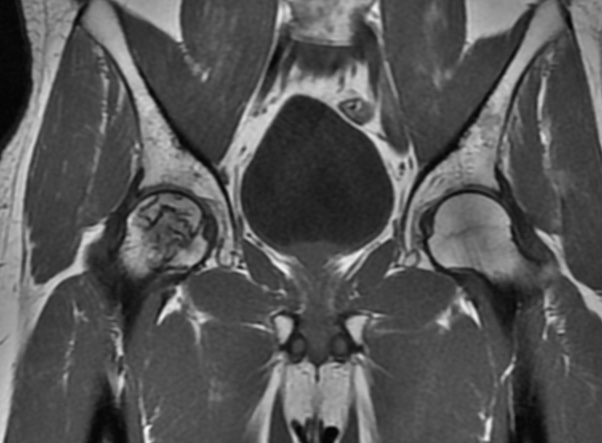
Sickle cell disease (SCD) is a genetic disorder that affects the shape of red blood cells and can cause various complications, including those affecting the cervical spine. MRI is a useful imaging modality for evaluating cervical spine involvement in SCD.
On MRI, cervical spine involvement in SCD may manifest as avascular necrosis (AVN) of the vertebral bodies, which is a result of ischemia and infarction of the bone marrow. This can lead to collapse of the vertebral body and subsequent compression of the spinal cord or nerve roots. AVN appears as areas of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, with associated bone marrow edema and enhancement of the surrounding soft tissues after contrast administration.
Additionally, SCD can cause cervical cord infarction, which may present as a high signal intensity on T2-weighted images in the affected area. Cervical cord infarction can also cause associated edema and swelling, resulting in spinal cord compression and potential neurologic deficits.
Other potential MRI findings in SCD may include disc herniation, spinal stenosis, and cervical myelopathy, which can be caused by various mechanisms related to the abnormal shape and function of red blood cells.
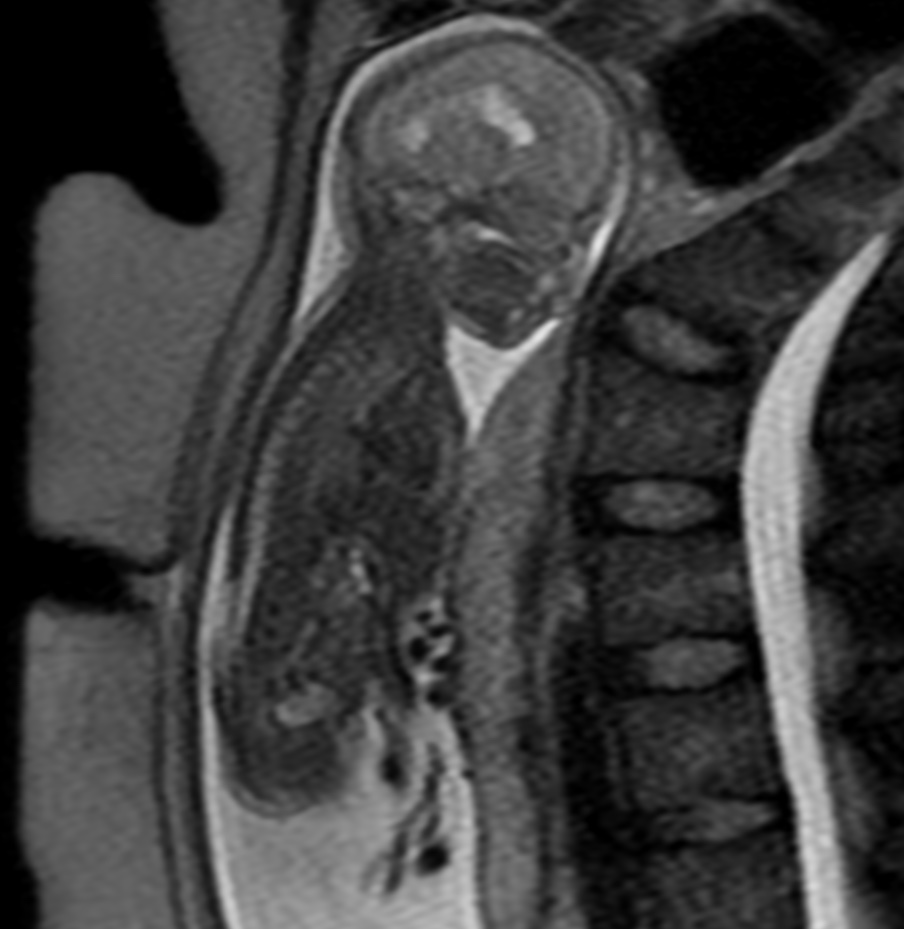
Chiari II malformation is a congenital anomaly of the brain that occurs due to incomplete development of the posterior fossa, leading to herniation of the cerebellar vermis and brainstem through the foramen magnum. Fetal MRI is a valuable imaging tool for detecting and characterizing Chiari II malformations prenatally.
On fetal MRI, Chiari II malformation typically appears as a downward displacement of the cerebellar vermis and brainstem through the foramen magnum. This results in a characteristic «banana sign,» which refers to the abnormal curvature of the brainstem and cerebellum. Additionally, there may be ventriculomegaly and aqueductal stenosis due to associated hydrocephalus.
Other findings on fetal MRI may include spinal dysraphism, such as myelomeningocele, which is present in up to 90% of cases. There may also be associated anomalies of the posterior fossa, such as absent or hypoplastic cerebellar hemispheres and vermis, and absent or hypoplastic fourth ventricle. These additional findings are important to consider in the overall management and prognosis of the affected fetus.
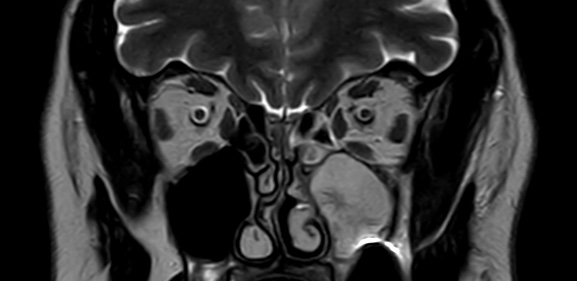
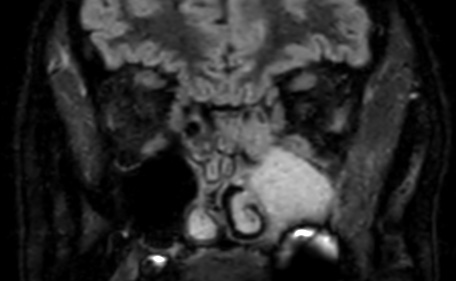
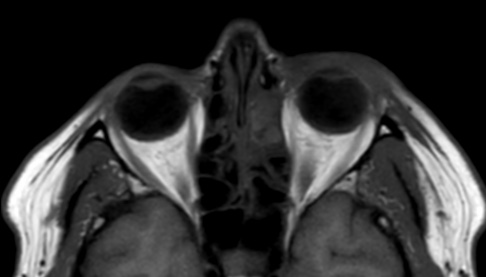
Orbital cellulitis is an infection of the soft tissues within the orbit (eye socket) of the skull. MRI is a useful imaging modality for evaluating orbital cellulitis due to its high resolution and ability to differentiate soft tissue structures.
On MRI, orbital cellulitis typically appears as a diffuse, ill-defined area of increased signal intensity on T2-weighted and fluid-attenuated inversion recovery (FLAIR) images, indicating edema and inflammation of the soft tissues within the orbit. There may also be associated enhancement of the affected tissues after intravenous administration of gadolinium-based contrast material.
In severe cases, MRI may also demonstrate abscesses or collections of pus within the orbit, which appear as areas of high signal intensity on T2-weighted and FLAIR images with associated rim enhancement after contrast administration.
Other potential findings on MRI may include proptosis, displacement of the extraocular muscles, and enlargement of the optic nerve sheath. These findings can help differentiate orbital cellulitis from other conditions that may present with similar symptoms, such as orbital tumors or Graves’ disease.
In summary, MRI findings of orbital cellulitis include a diffuse, ill-defined area of increased signal intensity on T2-weighted and FLAIR images, with associated enhancement of the affected tissues after contrast administration. Abscesses or collections of pus may also be seen in severe cases, along with proptosis, displacement of the extraocular muscles, and enlargement of the optic nerve sheath.
An intraventricular lipoma is a rare type of brain tumor that originates from fatty tissue within the ventricles of the brain. MRI is a preferred imaging modality for detecting intraventricular lipomas due to its high resolution and ability to differentiate soft tissue structures.
On MRI, an intraventricular lipoma appears as a well-circumscribed, homogeneous mass with low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, consistent with its fatty composition. The lipoma typically appears as a well-circumscribed, lobulated mass with a smooth contour, located within the ventricular system of the brain.
In addition, the MRI may reveal any associated hydrocephalus, which is an accumulation of cerebrospinal fluid within the brain, caused by obstruction of the normal flow of fluid due to the presence of the lipoma.
In summary, MRI findings of an intraventricular lipoma include a well-circumscribed, lobulated mass with low signal intensity on T1-weighted images and high signal intensity on T2-weighted images, with associated hydrocephalus if present.
In patients with sickle cell disease (SCD), the spine can be affected in various ways, including ischemic injury, bone infarction, and vertebral collapse. MRI is a useful imaging tool to detect these changes and assess the severity of spinal involvement.
The following are some common MRI findings in SCD patients with spinal involvement:
Vertebral compression fractures: These are common in SCD patients due to the weakened bone structure resulting from chronic anemia and ischemic injury. On MRI, vertebral compression fractures appear as wedged-shaped vertebral bodies with decreased height and abnormal signal intensity.
Bone infarction: This is a common complication of SCD that can affect the spine. On MRI, bone infarction appears as areas of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images.
Disk degeneration: Patients with SCD are more likely to develop disk degeneration due to the chronic anemia and ischemic injury. On MRI, disk degeneration appears as reduced disk height, loss of disk hydration, and bulging or herniation of the disk.
Vertebral collapse: In severe cases, SCD patients can develop vertebral collapse due to weakened bone structure. On MRI, vertebral collapse appears as a loss of vertebral height and increased signal intensity on T2-weighted images.
Spinal cord compression: In rare cases, SCD patients can develop spinal cord compression due to vertebral collapse or herniated disk. On MRI, spinal cord compression appears as a narrowed spinal canal and compression of the spinal cord.