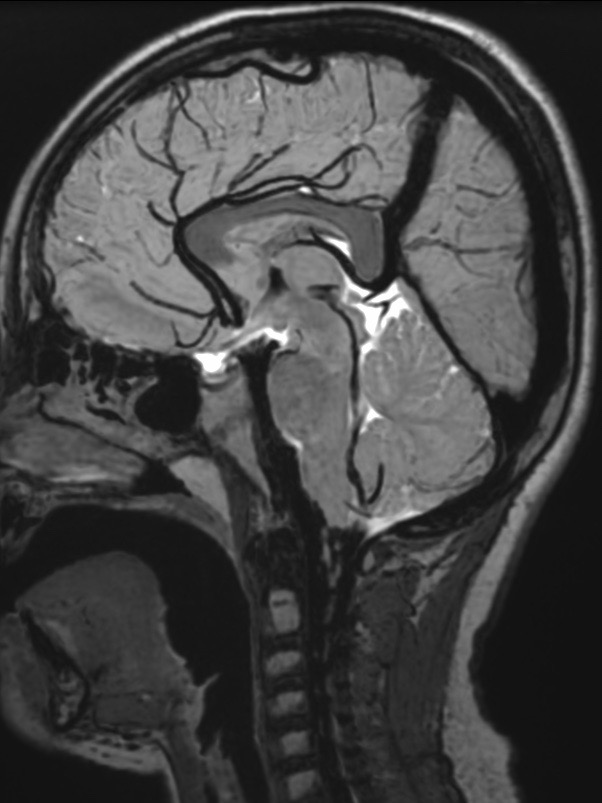
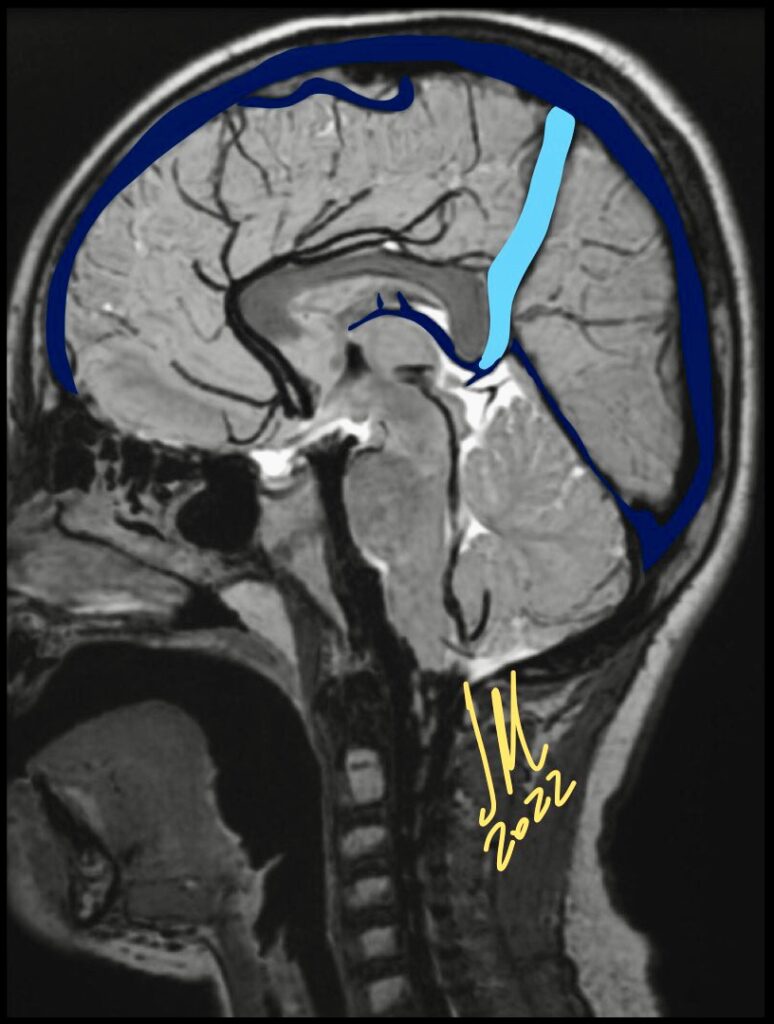
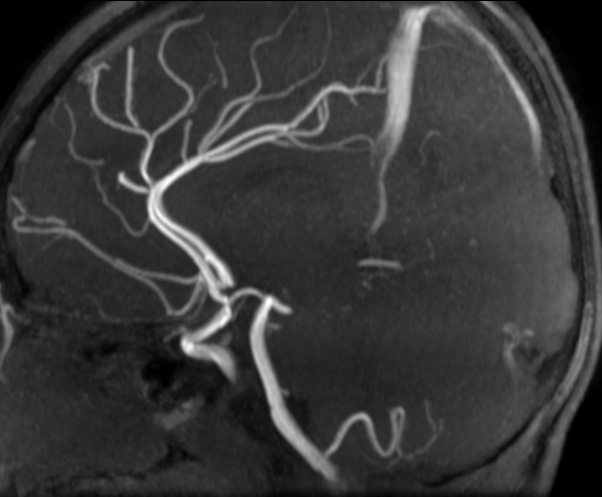
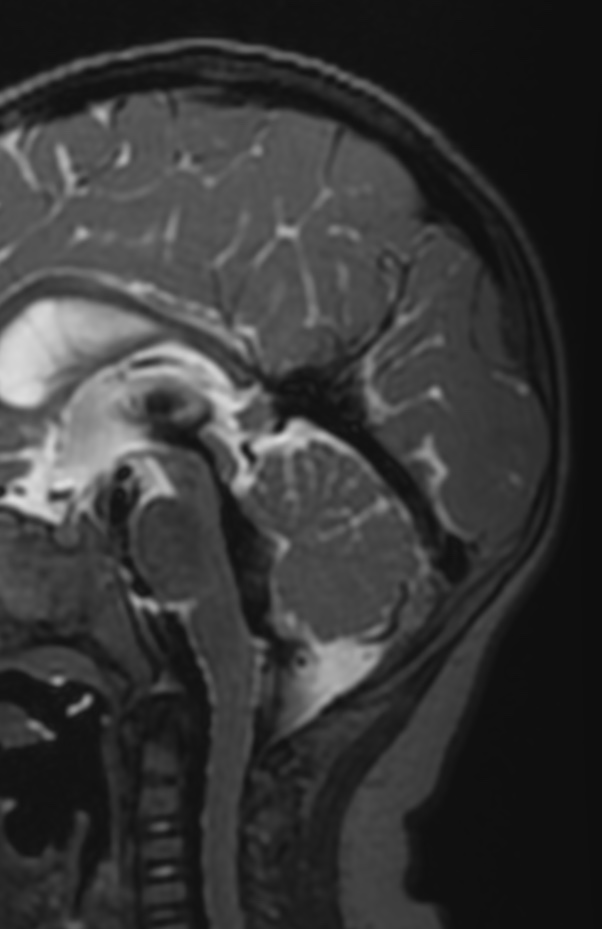
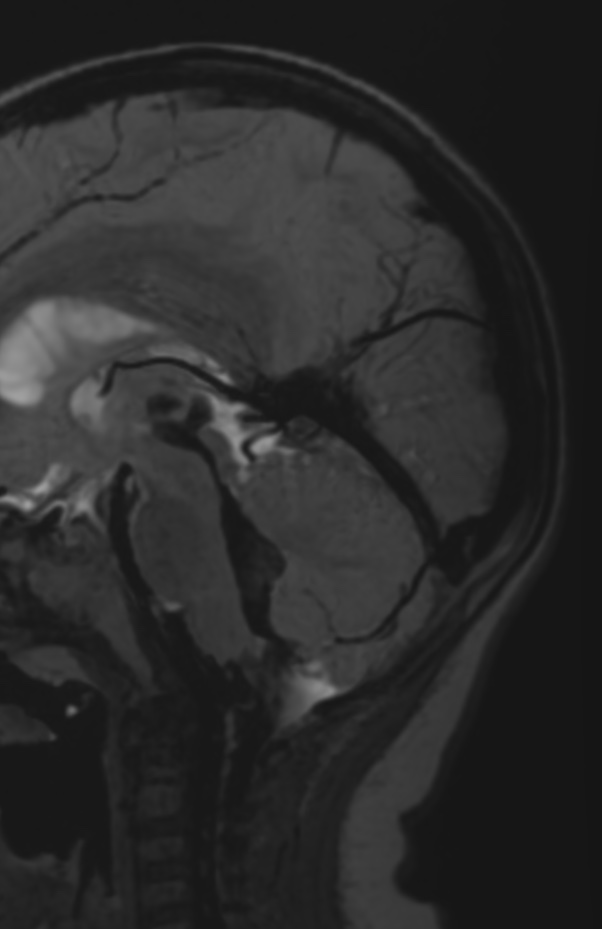
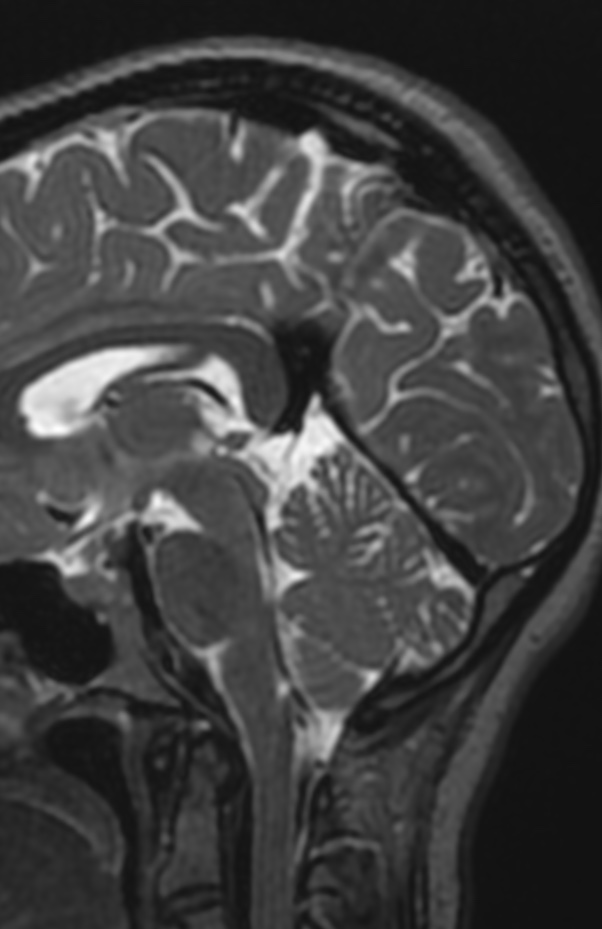
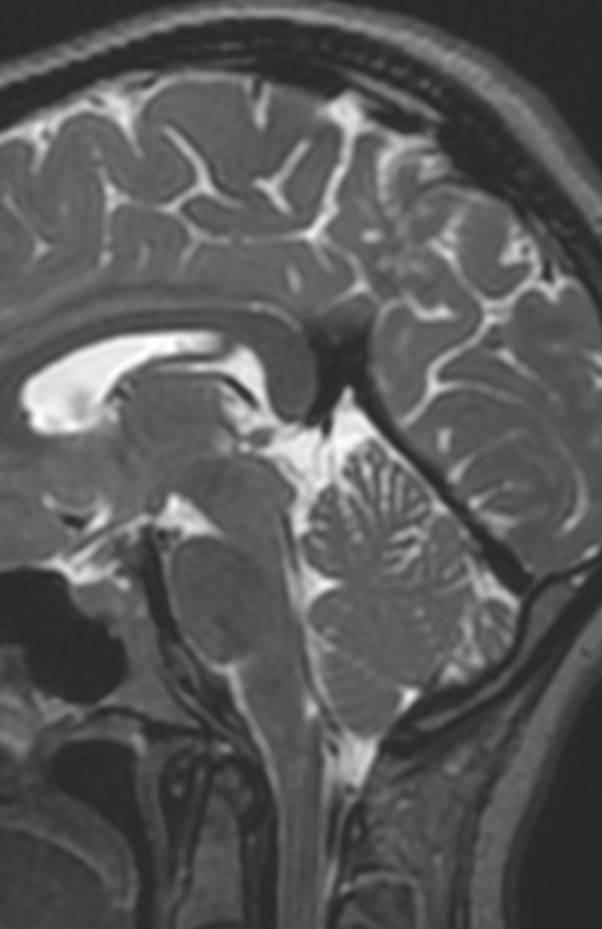
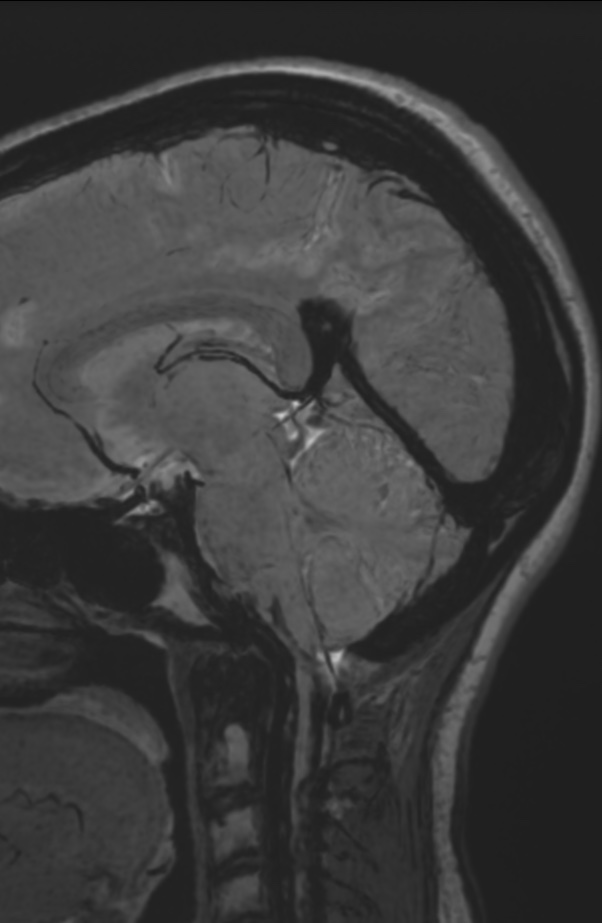
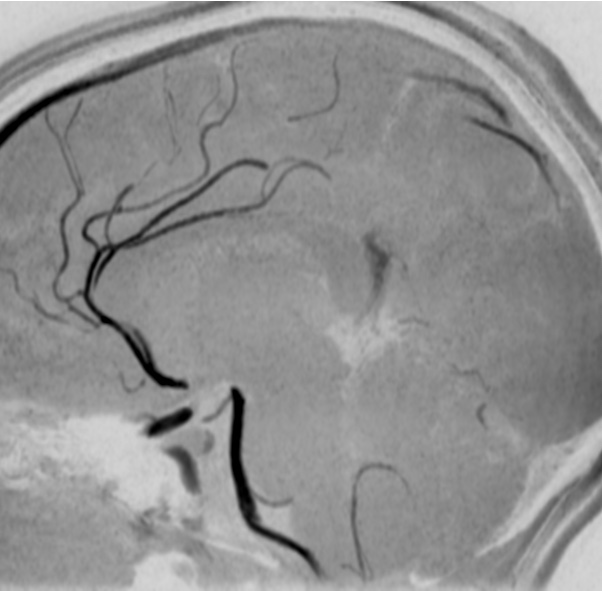
Persistent falcine sinuses are exceptionally rare and are typically present in the context of absent, hypoplastic, or occluded venous outflow tracts.This observation implies that alterations in cerebral venous flow dynamics may result in recanalization of the falcine sinus.
The falcine sinus is an embryonic venous structure in the falx cerebri that connects the vein of Galen to the superior sagittal sinus.
It normally closes before or shortly after birth. Persistent falcine sinus can be a congenital or acquired phenomenon related to a defect in the straight sinus that is thought to cause an alternative pathway to form for drainage from the deep to superficial venous system.
1Y. Hypoplasia1Y. hypoplasia
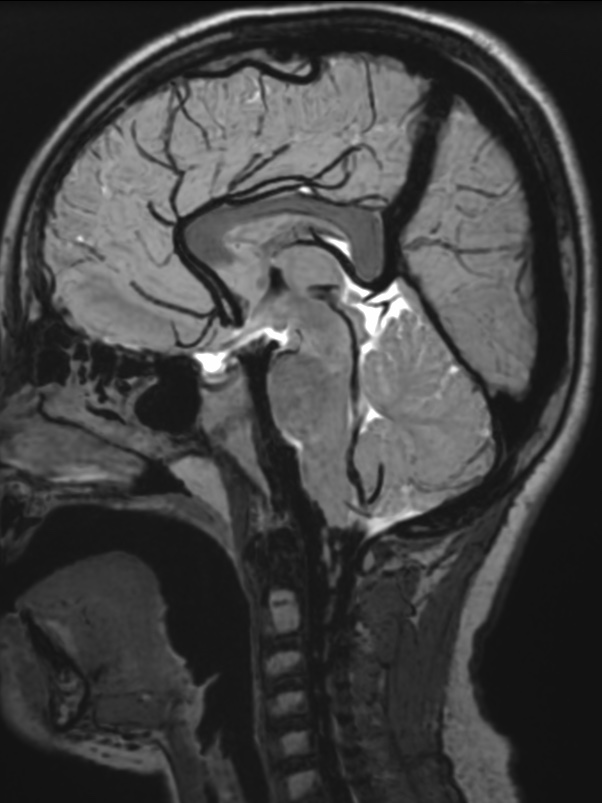
The falcine sinus normally closes before or shortly after birth. Congenital persistence of the falcine sinus is believed to be caused by a mesenchymal disorder that can also lead to hypoplasia or absence of the straight sinus. It may or may not be associated with other congenital anomalies of the brain.
Alternatively, persistent falcine sinus can be an acquired phenomenon with recanalization after thrombosis or obstruction of the straight sinus.
30Y Atresia30M Atresia
Once a persistent falcine sinus is identified, a thorough search for additional findings is imperative given the importance of early intervention in the developing brain.
Reference:
American Journal of Neuroradiology December 2020, 41 (12) 2351-2357; DOI: https://doi.org/10.3174/ajnr.A6816
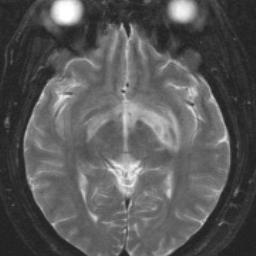
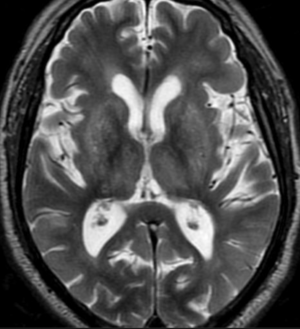
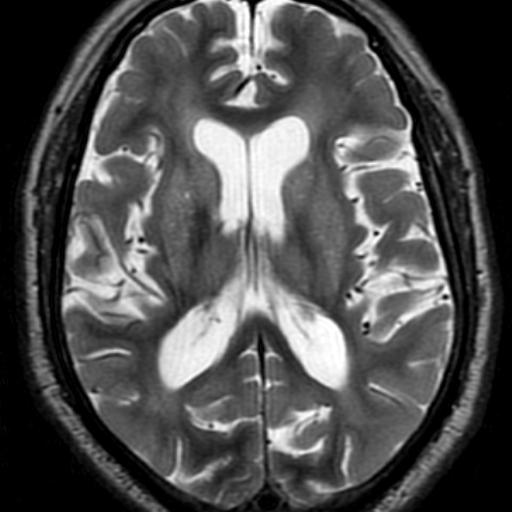
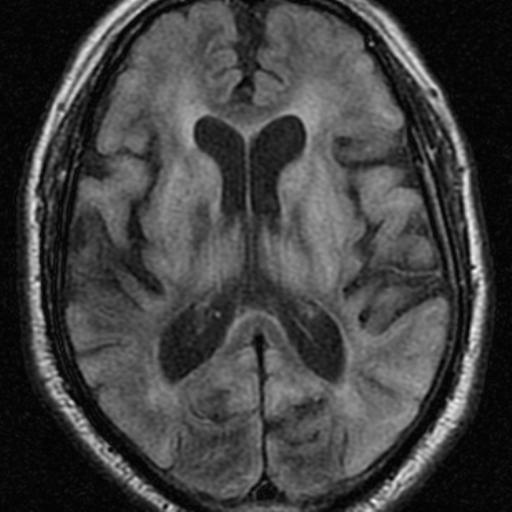
Hallervorden-Spatz disease now known as pantothenate kinase-associated neurodegeneration is a rare autosomal recessive neurodegenerative disorder associated with iron accumulation in the brain nuclei and characterized by progressive extrapyramidal dysfunction and dementia.
Is the standard in the diagnostic evaluation of all forms of Neurodegeneration with brain iron accumulation. It has significantly increased the likelihood of a diagnosis of PKAN.
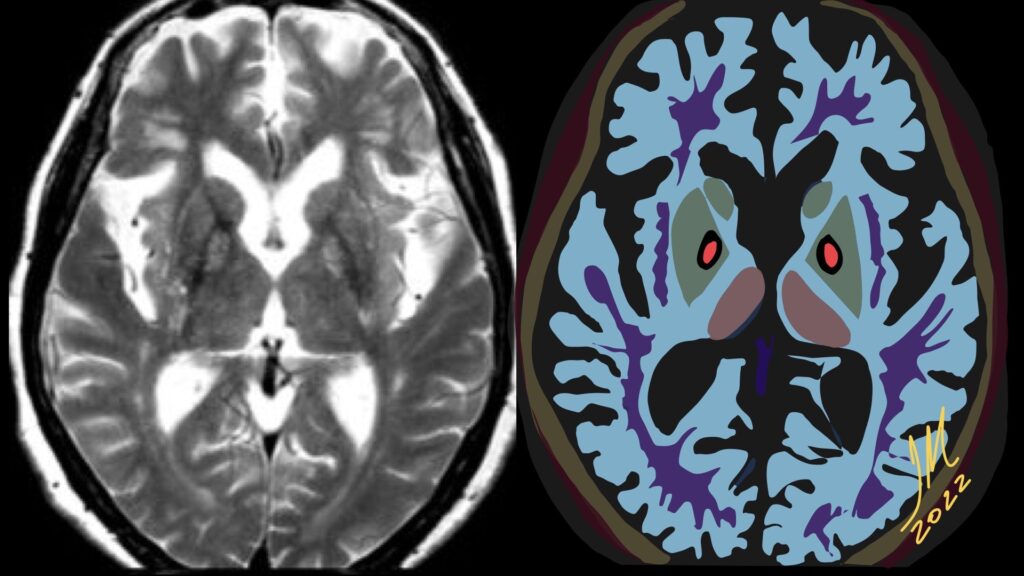
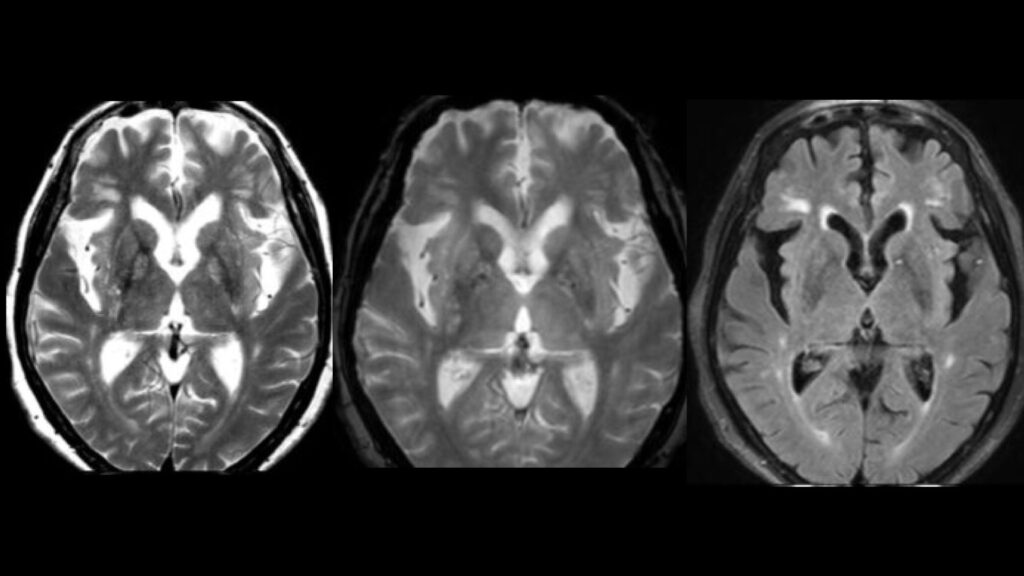
Imaging findings are most conspicuous on T2W-SWI-GRE sequences which demonstrate hypointensity reflecting areas of iron deposition, mainly in globi pallidi, pars reticulata of the substantia nigra, and red nuclei.
Studies report that all patients with PANK2 mutations, whether classic or atypical, have the characteristic radiologic sign known as «eye of the tiger» on brain MRI, which is evident as bilateral symmetrical, central foci of hyperintense signals in the anteromedial globus pallidus, with surrounding zone of hypointensity in the globus pallidus on T2W MR scanning. The central T2 relatively hyperintense spot or line within the globi pallidi is due to gliosis and vacuolation.
This sign was not reported in patients without PANK2 mutations. Cortex is usually spared, but atrophy can be seen in advanced cases. SWI-GRE Show susceptibility artifact (blooming low signal) in corresponding areas due to iron accretion. MR spectroscopy shows decreased NAA peak due to neuronal loss and may depict increased myoinositol.
Patients with mutations in the PANK2 gene can be distinguished from patients without the mutation by their specific brain MR imaging changes, even very early in disease.
Reference:
S.J. Hayflick, M. Hartman, J. Coryell, J. Gitschier and H. Rowley. American Journal of Neuroradiology June 2006, 27 (6) 1230-1233;
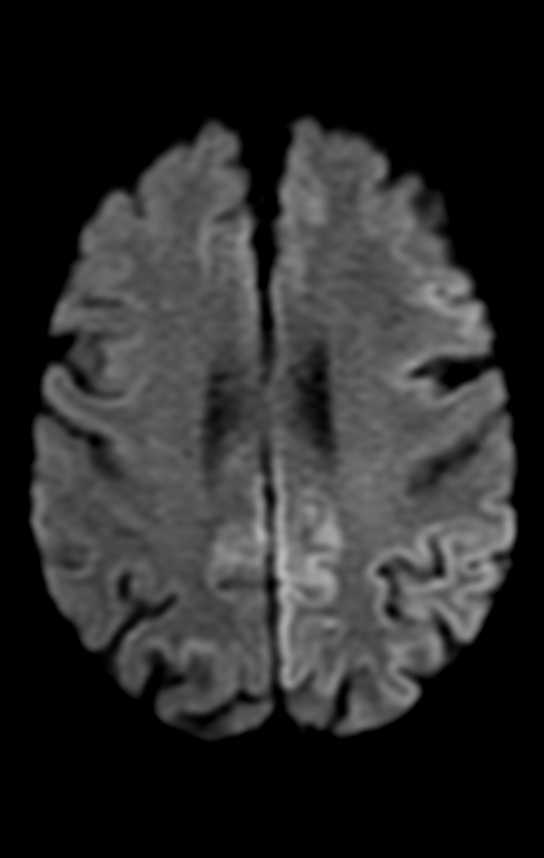
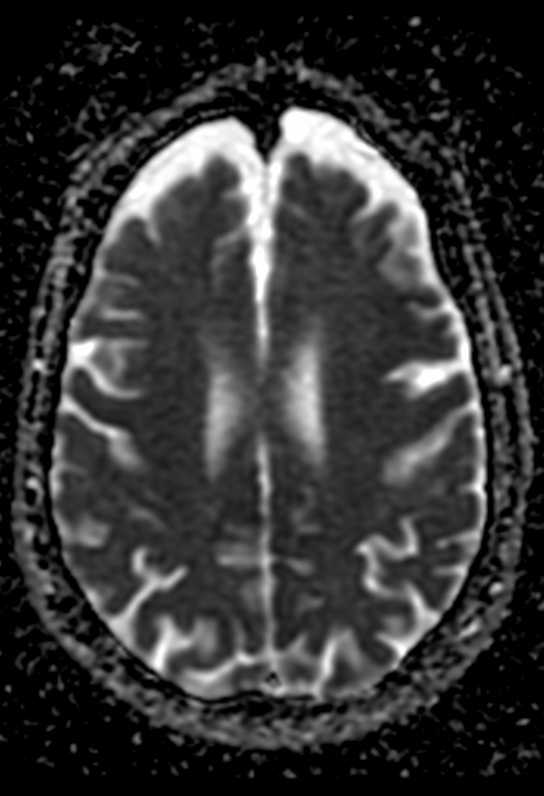
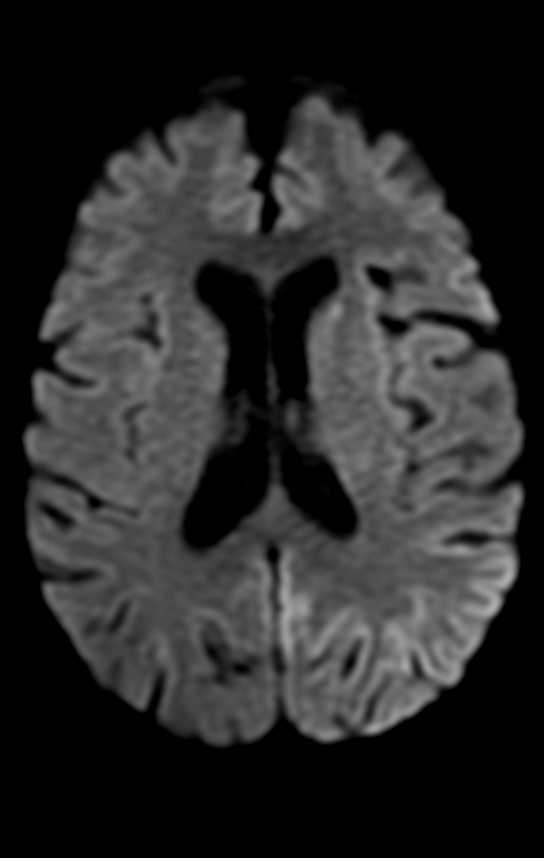
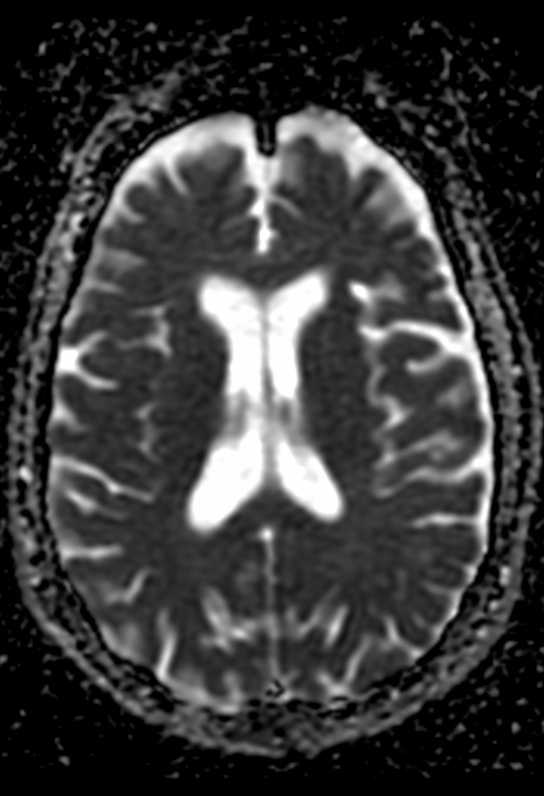
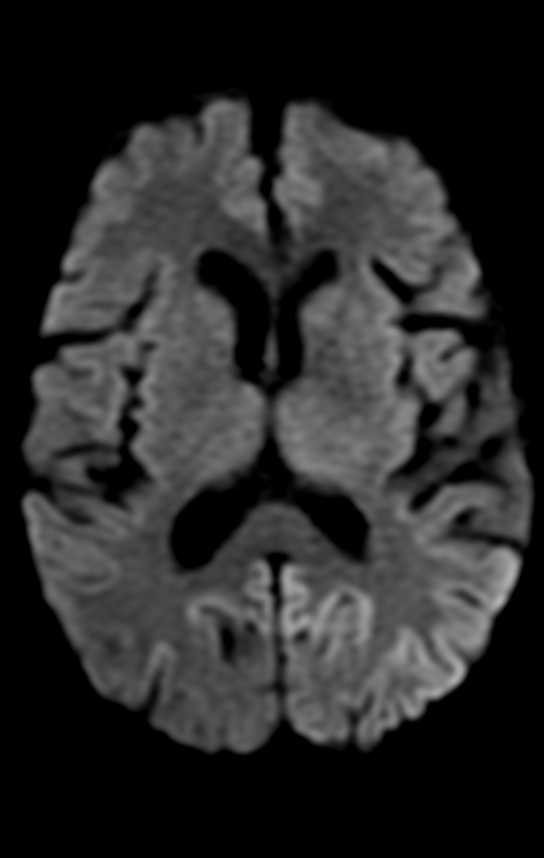
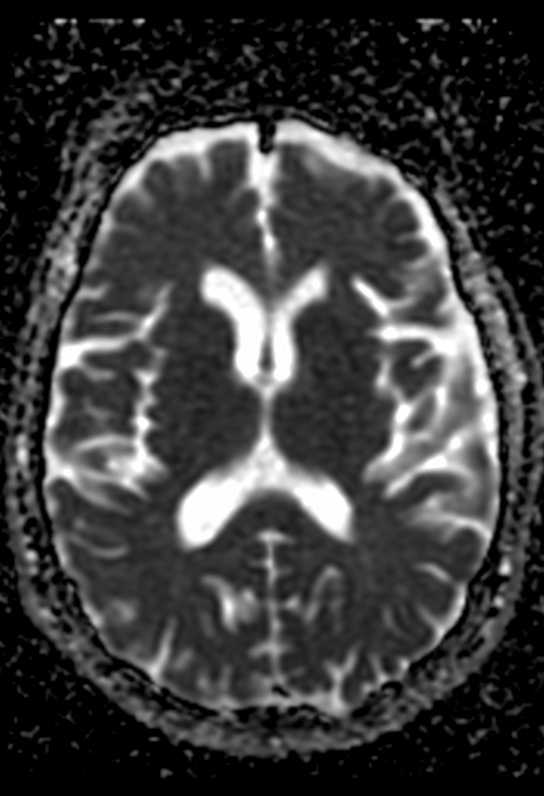
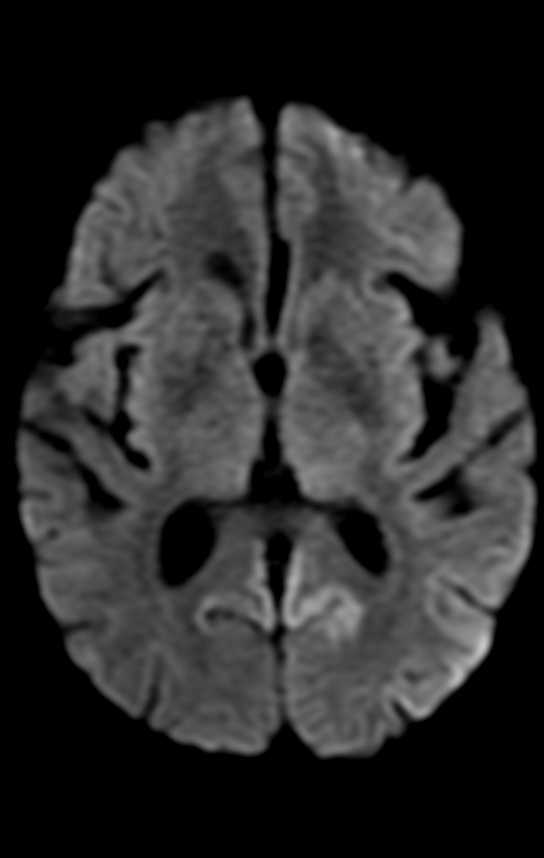
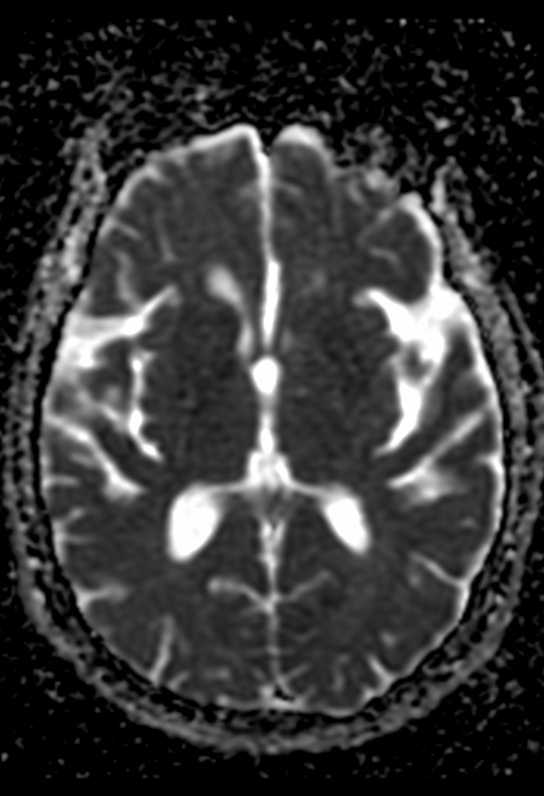
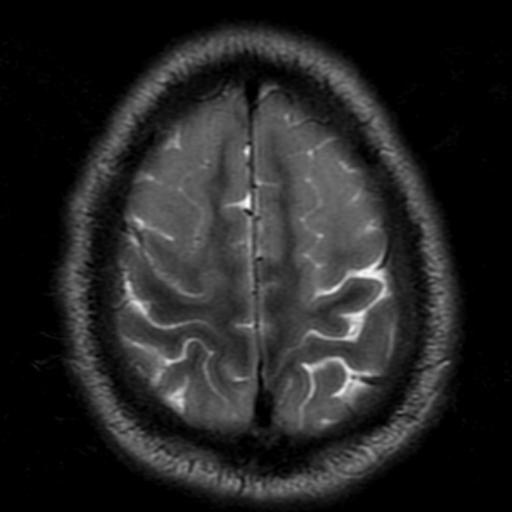
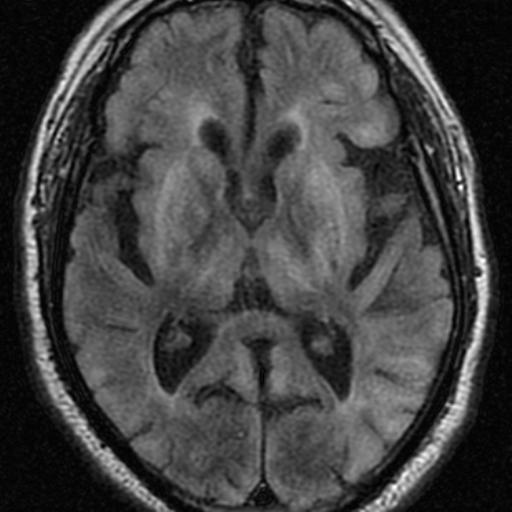
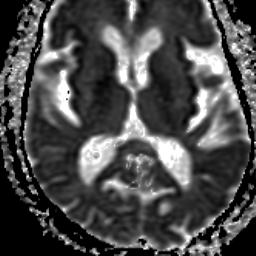
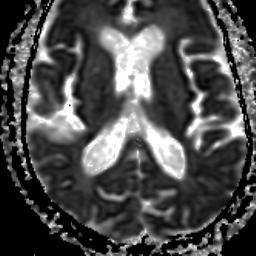
On MR imaging, the earliest changes are seen on DWI sequences. The involved regions show restricted diffusion with corresponding ADC hypointensity. The extent of these abnormalities depends on severity and duration of hypoglycemia.
Changes are usually bilateral, though bilaterally asymmetric, or, rarely, unilateral lesions, may occur. Reduction in ADC values has been shown to follow establishment of cerebral isoelectricity, a process that may be asynchronous. This may explain asymmetric lesions in a given patient.
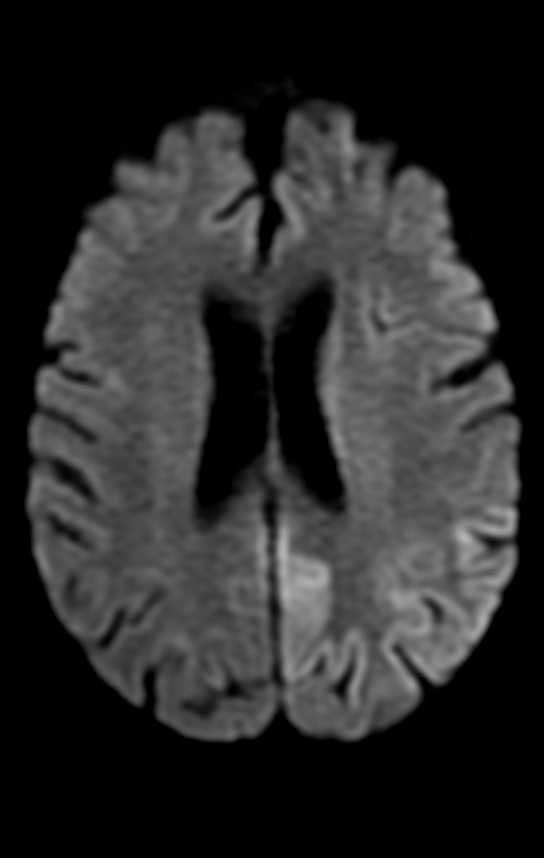
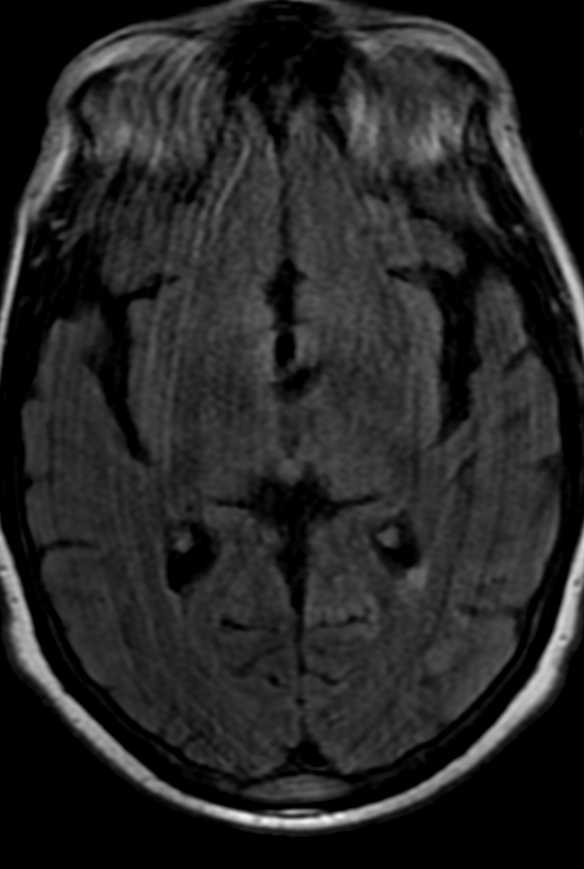
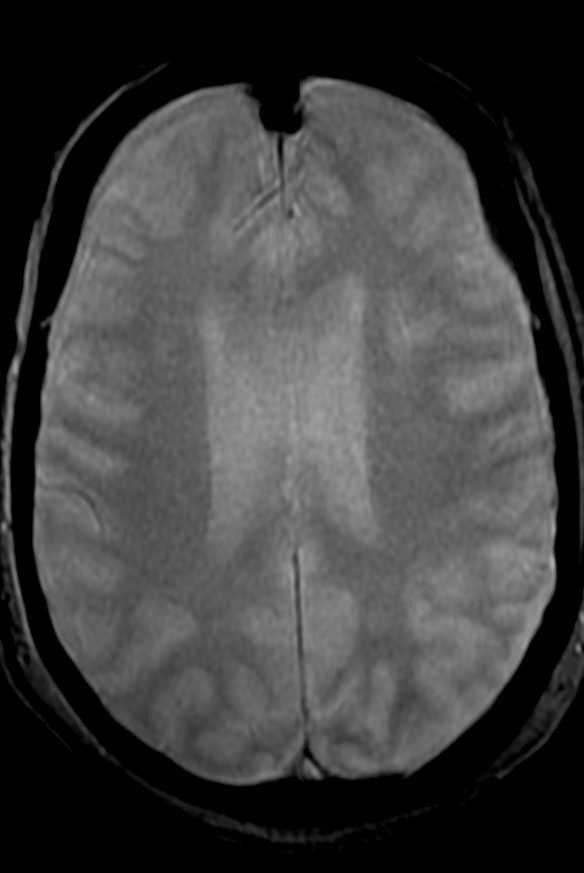
On the basis of the topographic distribution of the signal abnormalities, 3 imaging patterns have been described. These include 1) predominant gray matter involvement affecting the cortex, neostriatum, and hippocampi; 2) predominant WM involvement affecting the periventricular WM, internal capsule, and splenium of corpus callosum and 3) mixed pattern, involving both the gray matter and WM.
The division of patients on the basis of these imaging patterns is of unclear significance.Patients with focal involvement of the internal capsule, corona radiata, or splenium usually have a good prognosis. These lesions usually resolve promptly after restoration of blood glucose, though they tend to follow clinical symptom resolution. Resolution of DW abnormalities in their patient as early as 2 hours after blood glucose levels were restored.
Patients with extensive WM involvement show variable response. The prognosis in these cases varies between complete recovery and persistent vegetative state. Clinical improvement, if it occurs, is usually delayed by weeks.Involvement of the neostriatum and diffuse cortical lesions often portend dismal outcome. Failure of lesions to regress on follow-up imaging is also associated with poor prognosis.
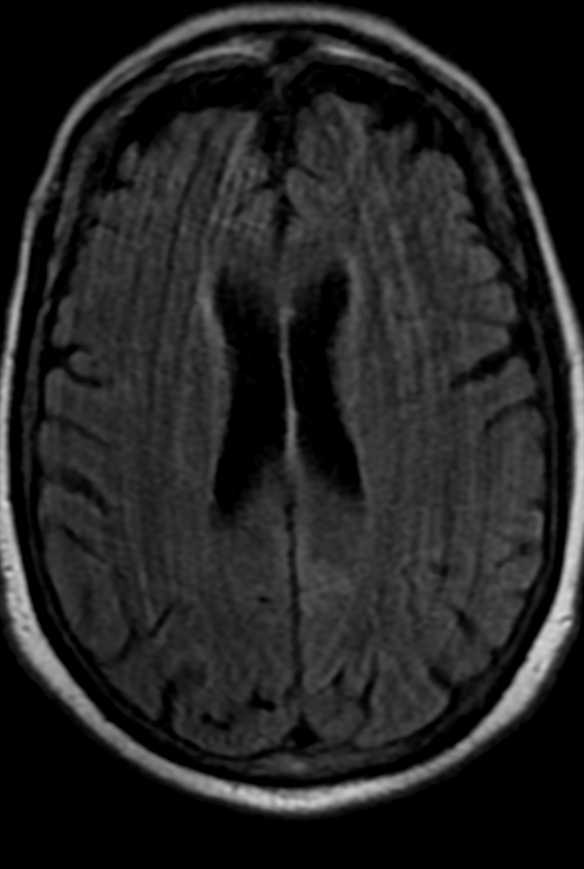
Findings of CT scans of the head on admission were often unremarkable in the reported cases, but in time, some acute-stage and chronic-stage changes have been demonstrated. In the acute stage, the changes varied from subtle decreased attenuation of the basal ganglia to diffuse brain edema, as severity of the hypoglycemia increased. In the chronic stage, diffuse brain atrophy and dilation of the ventricular system have been noted. MR imaging findings are comparable to the CT findings, mainly involving the cortex, internal capsule, basal ganglia, and hippocampus.
Diffusion-weighted MR imaging detects change in water diffusion with cellular dysfunction and primarily identifies early ischemic changes in stroke. Infarction is the most common cause of such a hyperintense lesion on diffusion-weighted imaging. In hypoglycemia, the incidence of cytotoxic edema, shrinkage of the extracellular space as a result of hypoglycemia, and failure of the ionic pumps cause the hyperintense lesion on diffusion-weighted MR imaging. ADC reductions similar to those seen after ischemia occur in hypoglycemia, status epilepticus, spreading depression, and excitotoxic brain injury, pathologic conditions characterized by a significant shrinkage of the extracellular space volume. However, status epilepticus and spreading depression in normal brain are conditions that are not associated with energy failure, and the ADC changes are reversible. Glucose deprivation leads to severe brain energy failure and a reduction of cell membrane ionic pump activity, as does anoxia/ischemia, but the topographic and temporal evolution of hypoglycemic brain damage is different from that of anoxia/ischemia.
Hyperacute short-term severe hypoglycemia for <10 minutes does not induce visible changes in DWI of the human brain, suggesting that prolonged hypoglycemia may be the relevant cause for observed reversible diffusion disturbances in MR imaging. Therefore, prompt adequate therapy for hypoglycemia can prevent cerebral injury in patients with diabetes.
Hypoglycemia was initially reported to predominantly involve the cortex, neostriatum, and hippocampus.However, many authors have also reported predominant WM involvement, mainly affecting the centrum semiovale, corona radiata, internal capsule, an splenium of the corpus callosum.In fact, involvement of the WM is now thought to be earlier and more common than gray matter involvement. Some cases may show diffuse gray matter and WM involvement. The thalamus, brain stem, and cerebellum are invariably spared, and this may help to differentiate hypoglycemia from hypoxic injury, which often involves the thalamus.
Hypoglycemia is more common in diabetic patients and can occur as a complication of therapy with insulin or long-acting sulfonylurea drugs. Other causes include exogenous administration of insulin, which may be suicidal or accidental, insulin-secreting tumors, sepsis, Addison disease, and hepatic or renal failure.
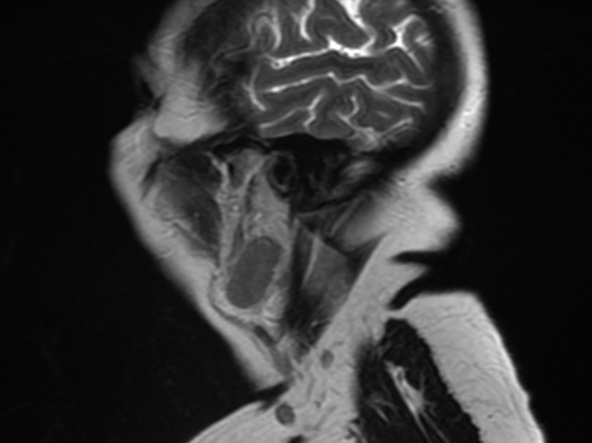
Themamillopontine distance or pontomamillary distance is defined as the distance between mamillary bodies to the superior aspect of the pons. When the mamillopontine distance is less than 5.5mm, it is an important indicator to diagnose intracranial hypotension.
Intracranial hypotension can be a challenging diagnosis because of the varied spectrum of clinical symptoms and is sometimes misdiagnosed as migraine headaches, meningitis, or a psychogenic disorder which can delay effective treatment.
the cause of intracranial hypotension may be identifiable, such as a sequela of trauma from skull base or facial fracture, craniospinal surgery, or lumbar puncture.
The clinical hallmark of intracranial hypotension is orthostatic headache.
Imaging is a critical part of identifying the diagnostic criteria for intracranial hypotension. There are five typical but variably present imaging characteristics: dural (pachymeningeal) enhancement, venous engorgement, pituitary hyperemia, subdural collections, and brainstem slumping.
Reference:
DOI:10.2214/AJR.12.8611 Intracranial Hypotension: Improved MRI Detection With Diagnostic Intracranial Angles
Rezaee, A., Smith, D. Mamillopontine distance. Reference article, Radiopaedia.org. (accessed on 31 Mar 2022) https://doi.org/10.53347/rID-43163
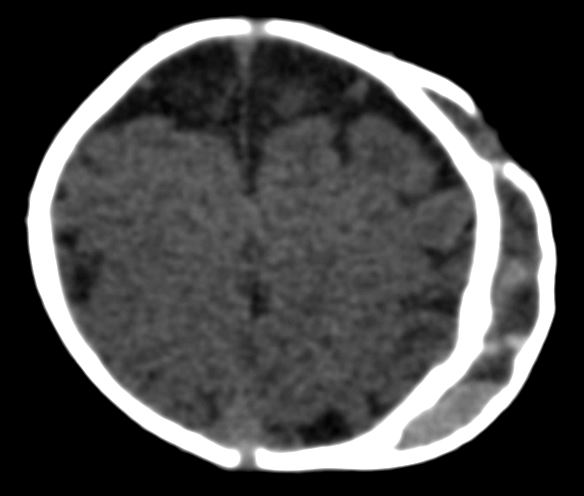
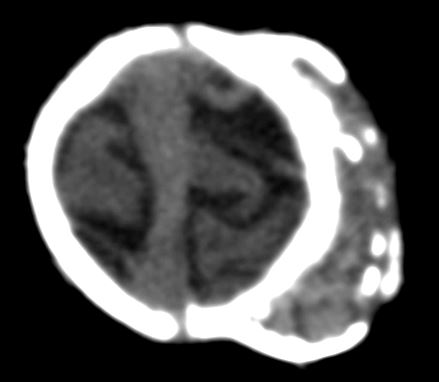
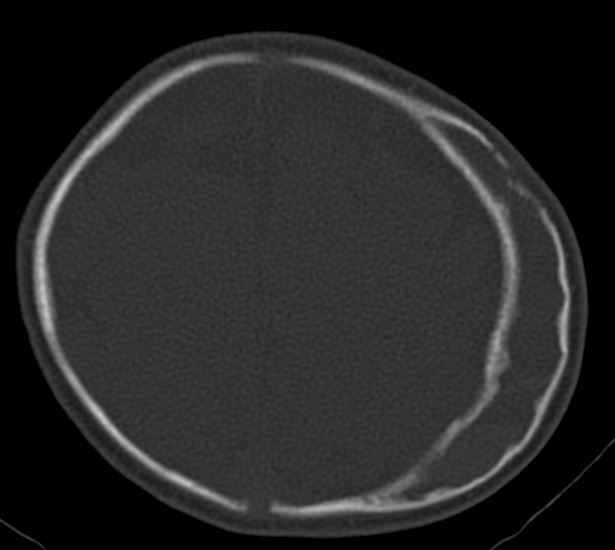
Calcified cephalohematoma of infancy is a result of a subperiosteal blood collection, that usually forms during birth-related trauma. It occurs when a cephalohematoma is not absorbed within the first weeks of its presentation and begins to ossify over the surface. The calcification may continue to enlarge. Calcification occurs in <5% of cephalohematomas.
Calcified cephalohematomas can permanently deform the infant cranium, and significant deformities often require correction. Although several reconstructive techniques have been proposed, there is no consensus on their management.
Images courtesy Dr. Andres Agudelo. Universidad Pontificia Bolivariana
Reference:
Management of Calcified Cephalohematoma of Infancy: A Single Institution 25-Year Experience University of Michigan – C. S. Mott Children’s Hospital, Ann Arbor, MI doi: 10.1097/01.GOX.0000720480.19319.a0
Al Kabbani, A., Bell, D. Calcified cephalohematoma. Reference article, Radiopaedia.org. (accessed on 30 Mar 2022) https://doi.org/10.53347/rID-72946
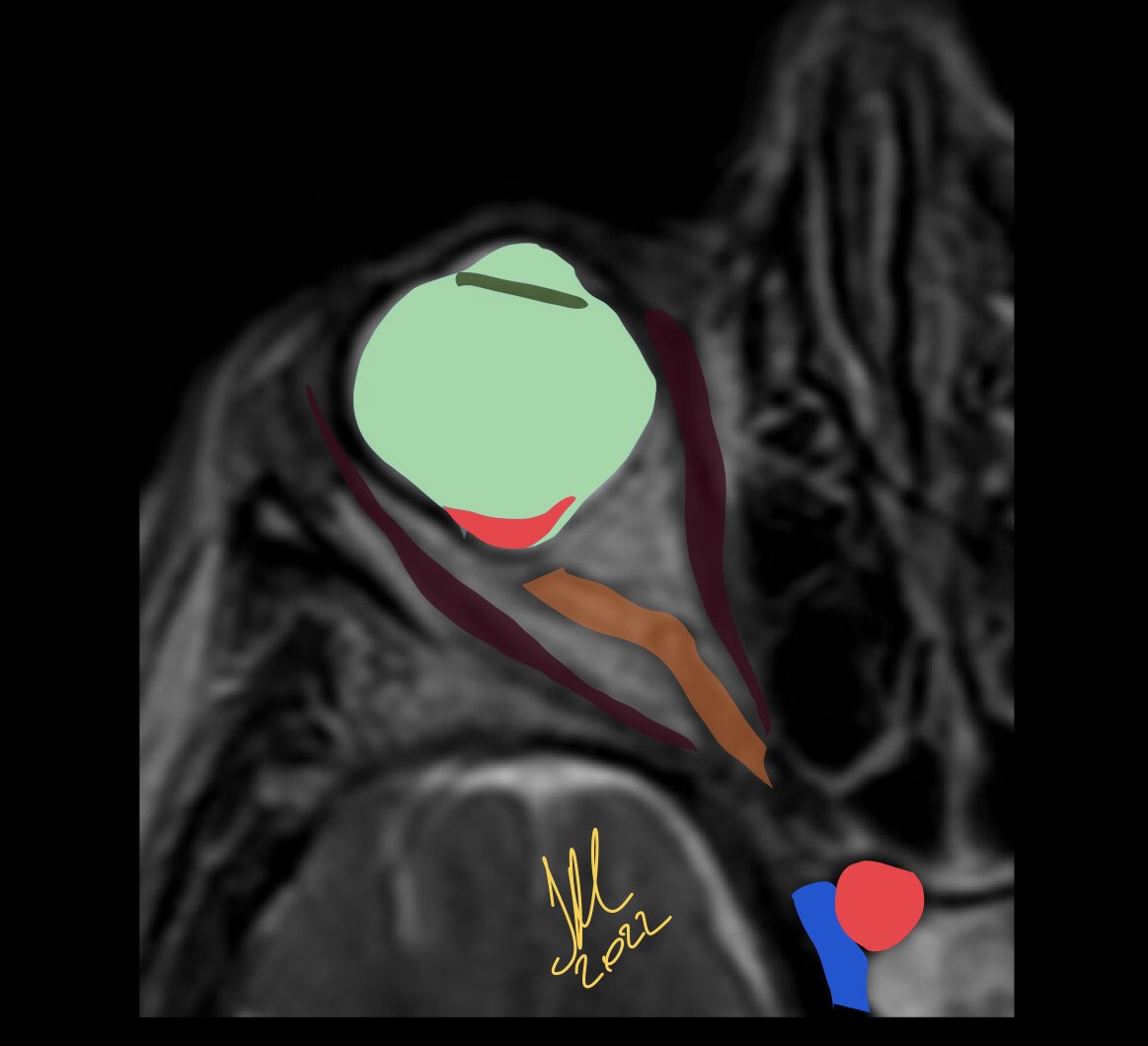
Posterior staphyloma is sine qua non of pathological myopia. It is characterized by disproportionate scleral ectasia with stretched conforming retinochoroidal layers. Conventionally, it has been classified into multiple types depending on location, although it usually involves the posterior pole of the eye. This outbulge, however, is a major risk factor for visually impairing maculopathy. PS can also be seen independent of high axial myopia.
As opposed to coloboma, staphyloma defect is located off-center from the optic disc, typically temporal to the disc.
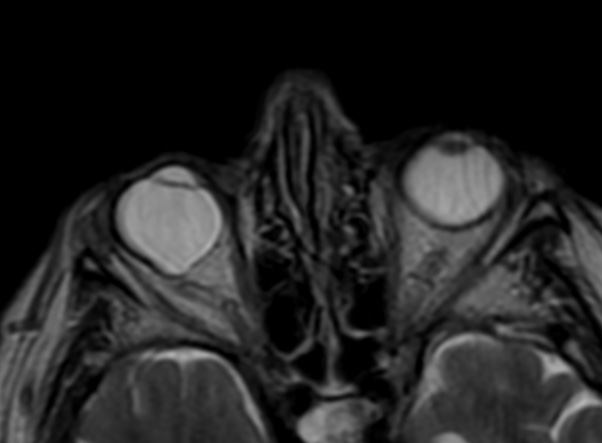
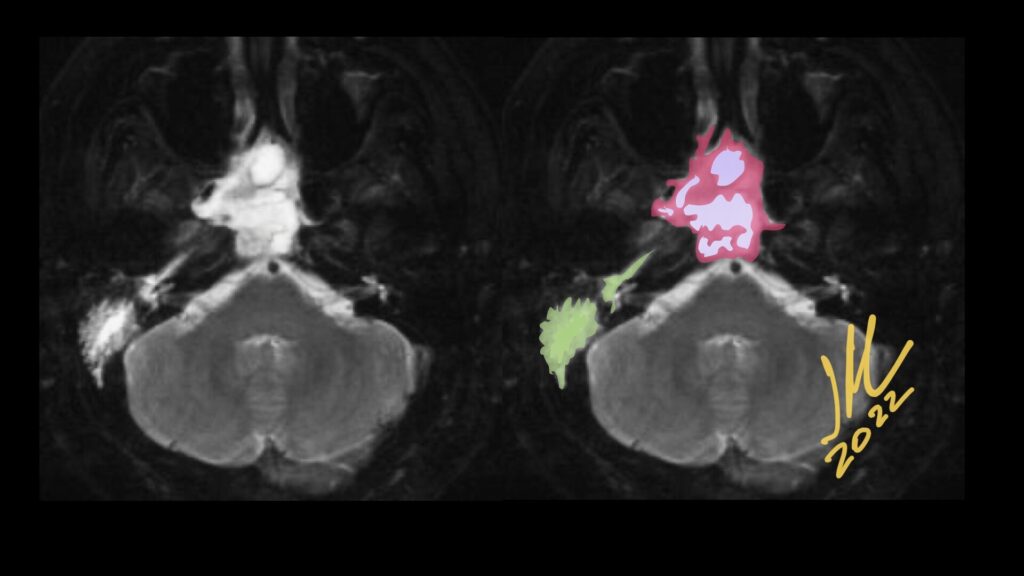
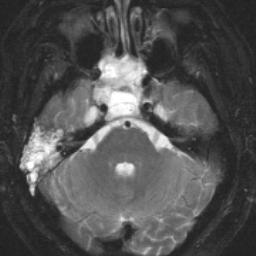
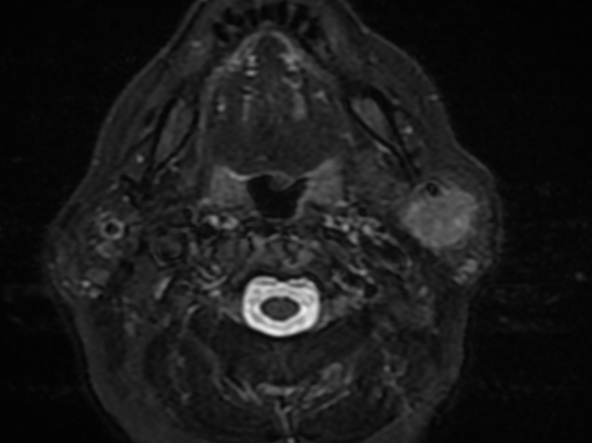
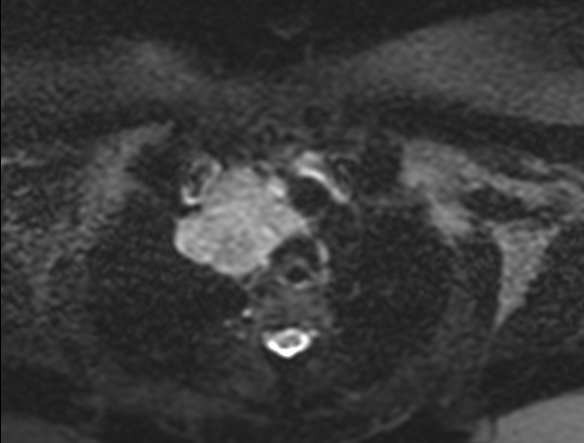
Primary nasopharyngeal adenoid cystic carcinoma (NACC), classified as a pathological type of adenocarcinoma, is a rare epithelioid malignancy that represents only 0.13% of all nasopharyngeal malignancies, but occurs most frequently in the salivary glands.
The main radiological characteristic is the tendency to perineural spread.
NACC lesions are located in the submucosal space of the pharyngonasal cavity without a well-defined boundary. Patients show masses with several obviously lobulated shapes, spreading along the interspaces around the cavity. the extension patterns and just characterized NACC as slow growth, frequent local recurrence, and metastatic spread.
the appearance in MR are isointense on T1, hyperintense-isointense on T2 and significantly contrast enhanced.
NACC is a malignant epithelial tumor of the salivary glands, occurring most frequently in the 5th decade of life, without sex predilection. It is the most common malignancy of the submandibular and minor salivary glands.
In the nasopharynx, NACC can vary in presentation from an asymptomatic mass to severe ear and neurological symptoms, such as ear pain, fullness, tinnitus, hearing loss, facial pain, unilateral migraine-like headache, paresthesias, numbness, sensory loss across the trigeminal nerve course, abducens or oculomotor nerve deficits.
Dong J, Zhang L, Mo Y, Tian L, Liu L, Wu P. Discovery of Invasion Routes for Nasopharyngeal Adenoid Cystic Carcinoma. J Cancer 2015; 6(1):90-97. doi:10.7150/jca.10739. Available from https://www.jcancer.org/v06p0090.htm
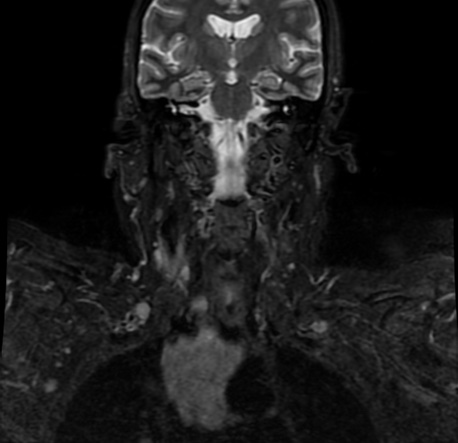
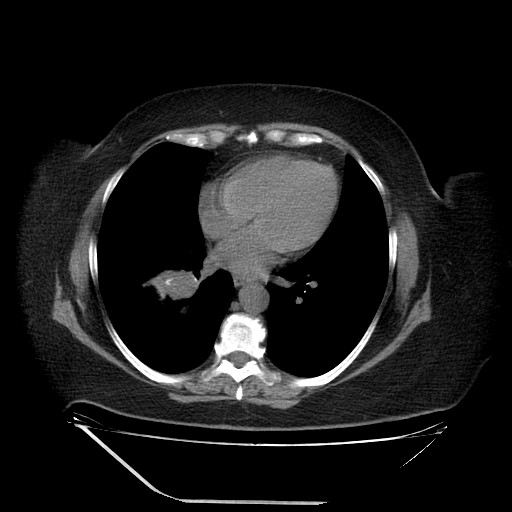
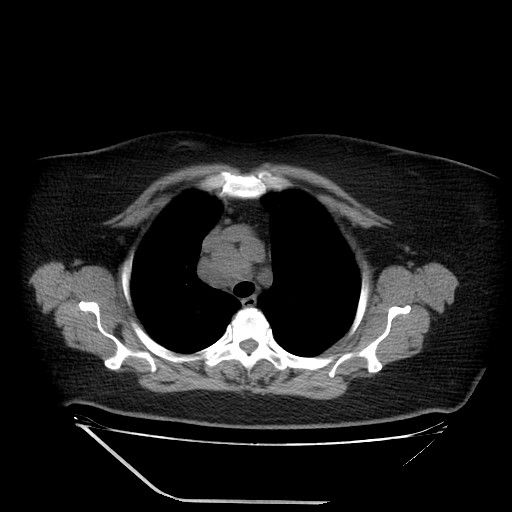
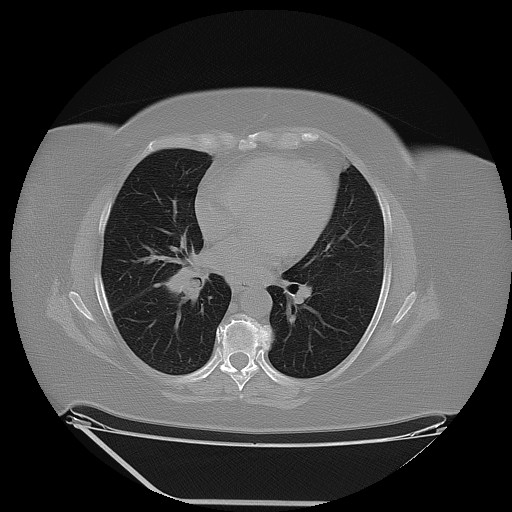
Parotid gland is an uncommon metastatic site for non-head and neck primary tumours. Metastatic tumours found in the parotid gland more commonly originate from primary head and neck cancers, while those originating from non-head and neck sites constitute 13% of metastatic lesions found in the parotid. Of the various non-head and neck primary tumours, lung cancer is the most common site of origin with other previously reported sites include renal, breast, colon and gynaecological carcinomas, as well as lymphomas.
It is postulated that these infraclavicular tumours usually affect the parotid parenchyma by means of haematogenous spread, while primary head and neck malignancies tend to spread to the parotid lymph nodes via the lymphatics.
MTS involving males with a median age of 60 years (range 40–74 years).
Although it is extremely rare, a potential metastasis of lung cancer should not be ignored in the diagnosis of a parotid tumor. Preoperative routine examinations such as a chest X-ray and lung CT, may play an important role in the differential diagnosis.
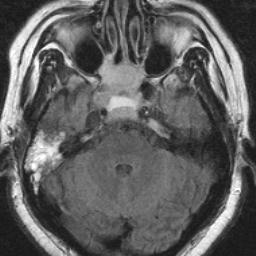
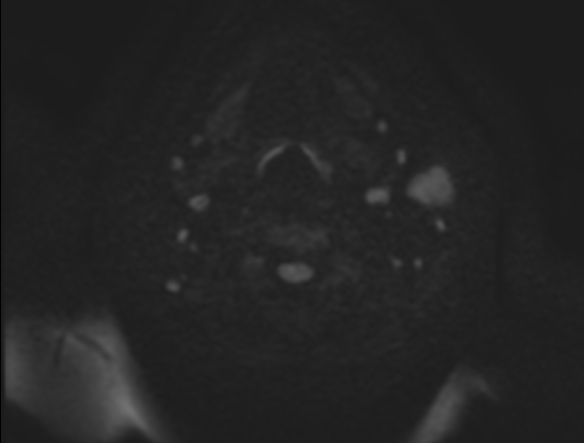
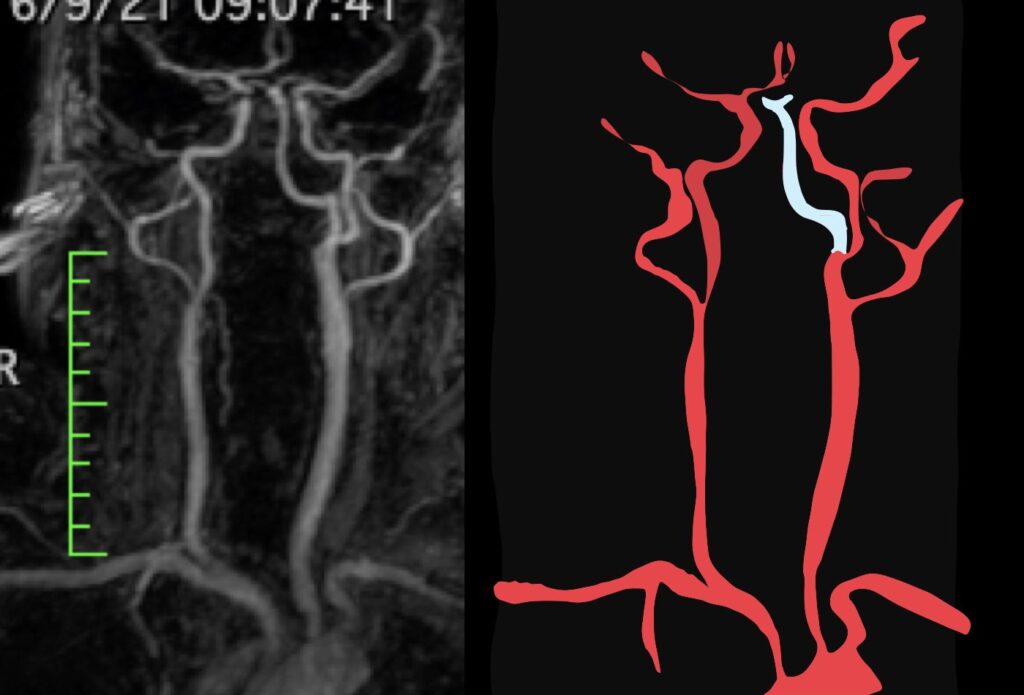
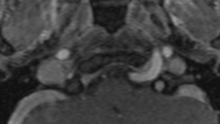
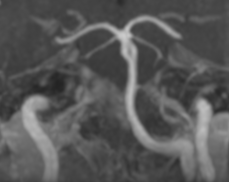
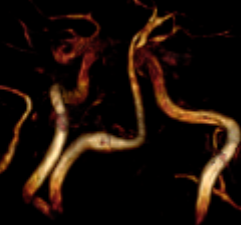
The persistent hypoglossal artery is the second most common carotid-basilar anastomosis. the prevalence is 0.1% to 0.2%. the primitive hypoglossal artery originates from the cervical part of the internal carotid artery at the level of C-1 to C-3.
After a tortuous course, it penetrates the enlarged hypoglossal canal and joins the lower portion of the basilar artery. When it is large, the proximal vertebral arteries usually are hypoplastic and the ipsilateral vertebral artery may be absent. the persistent hypoglossal artery is more frequent in females and on the left side as in our case.
The proatlantal intersegmental artery enters the posterior fossa through the foramen magnum, following the course of the vertebral artery. Therefore, differentiation between these primitive arteries on MR will be easy by demonstrating the foramen through which it passes.
This vascular anastomosis may be of functional importance in patients with carotid stenosis and may provide a pathway for cerebral embolism.
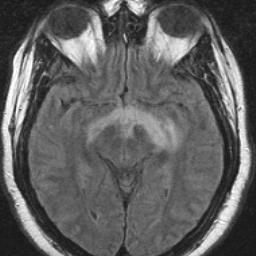
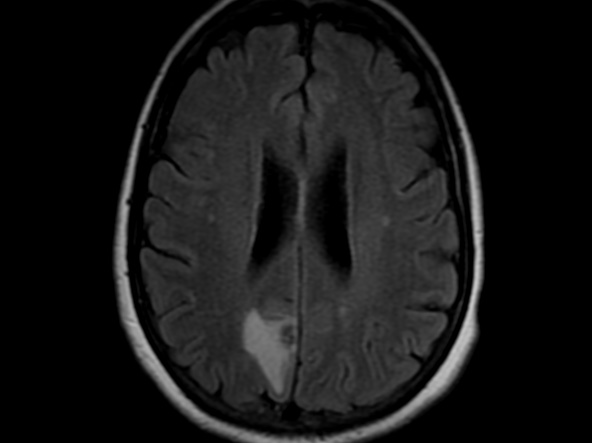
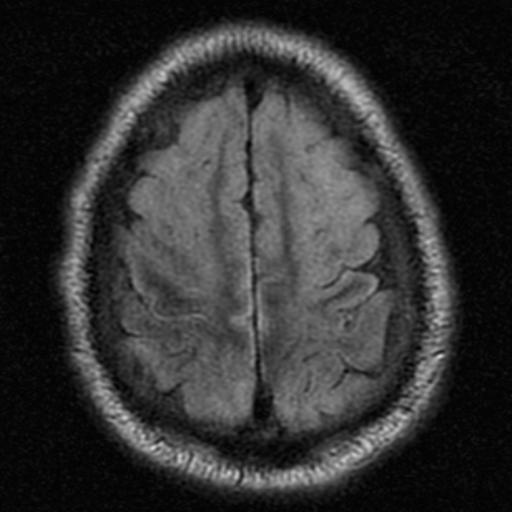
Hypoxic-ischemic encephalopathy (HIE) is the result of decreased global perfusion or oxygenation. The distribution of HIE varies according to the duration, degree, and abruptness of the hypoxic and/or ischemic insults, basal blood low, and metabolic activity in the areas of ischemia, temperature, and serum glucose levels. Layers 3, 4, and 5 of the cortex, watershed zones, and the hippocampi (cornu ammonis 1 zone) are sensitive to ischemia. DW hyperintensity throughout the cerebral cortex suggests devastating diffuse hypoxic-ischemic necrosis, whereas a pattern of basal ganglia or thalamus suggests primary hypoxic injury or mild HIE. Imaging Features include; Symmetric T2/FLAIR hyperintensity in deep gray nuclei and cortex.
The location of the injury correlates with the severity; mild to severe> Watershed zone infarcts, Gray matter, basal ganglia, sensorimotor and visual cortex, cerebellum( in older patients)and hippocampi.
Reference:
Diffusion-Weighted MR Imaging of the Brain Moritani . Ekholm . Westesson. P- 172