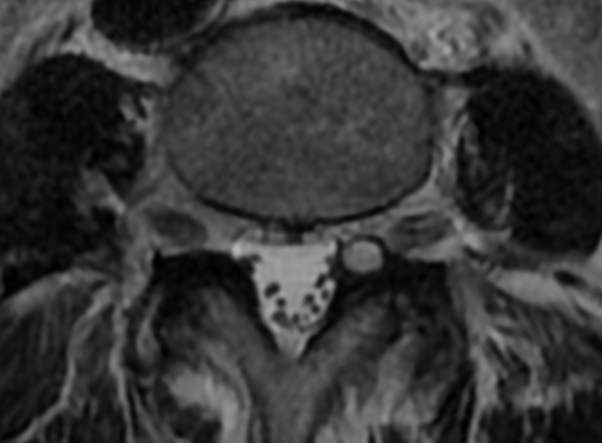
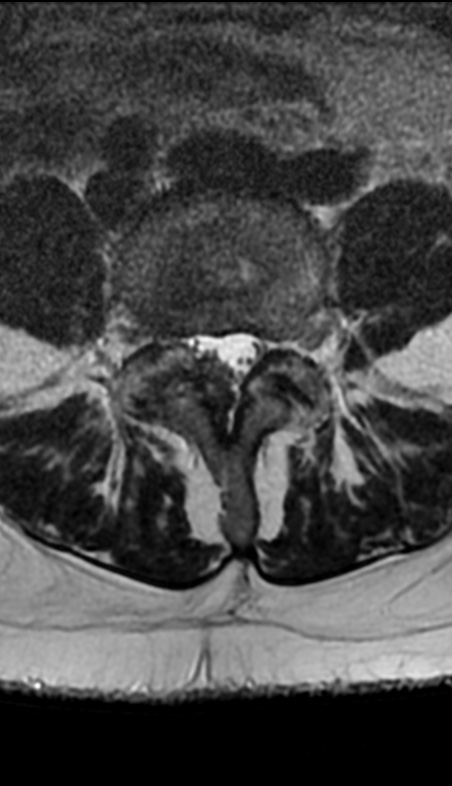
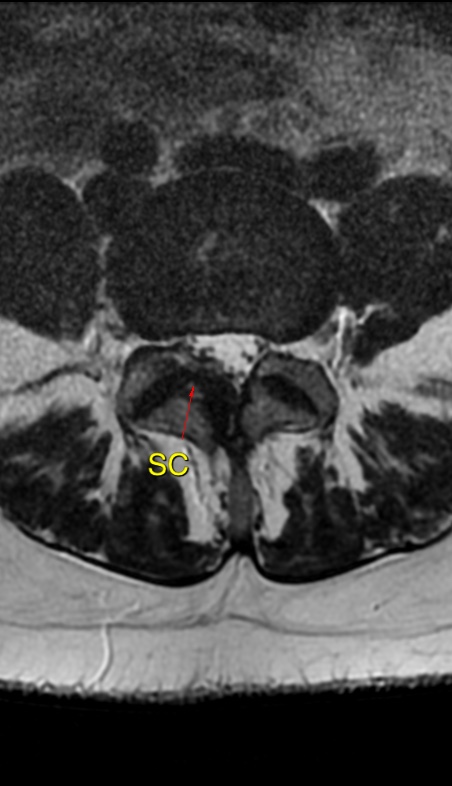
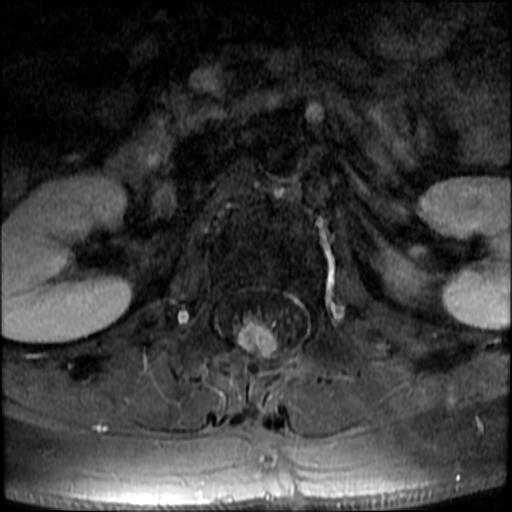
SCs are herniations of the synovial membrane through the capsule of a joint filled by synovial fluid, which may or may not keep a communication with the joint.
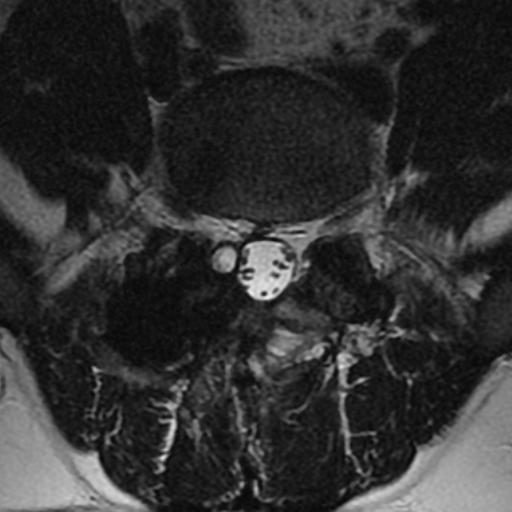
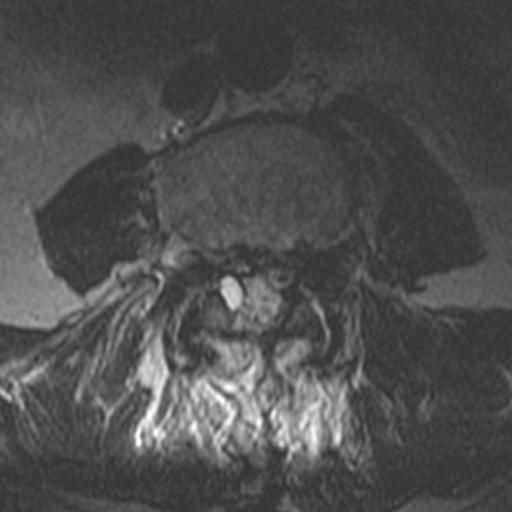
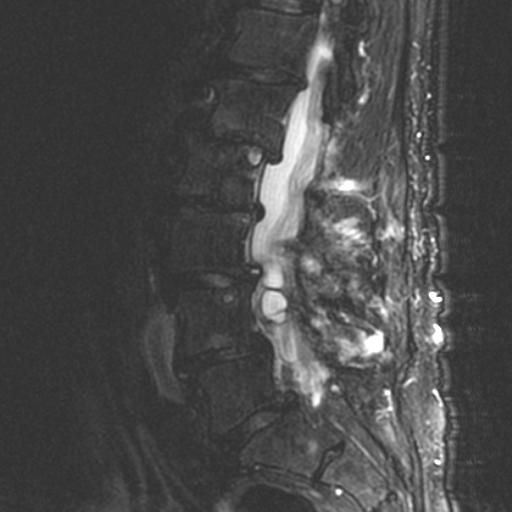
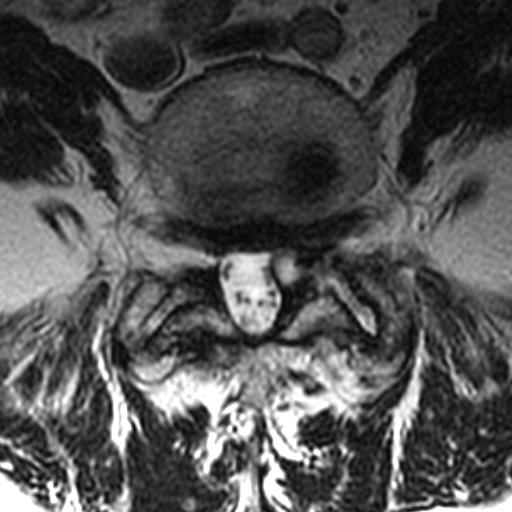
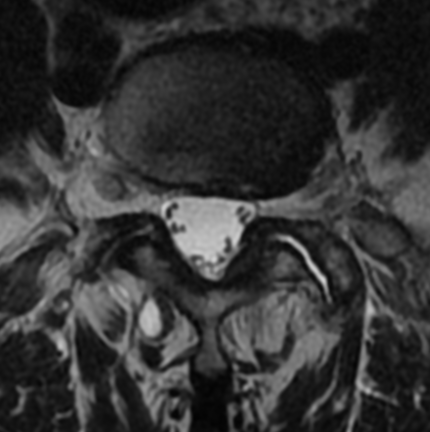
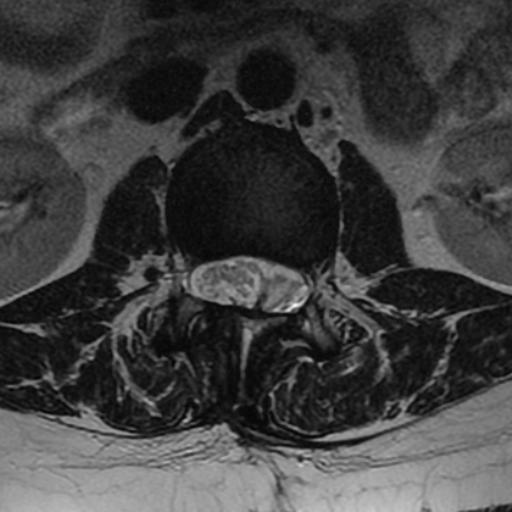
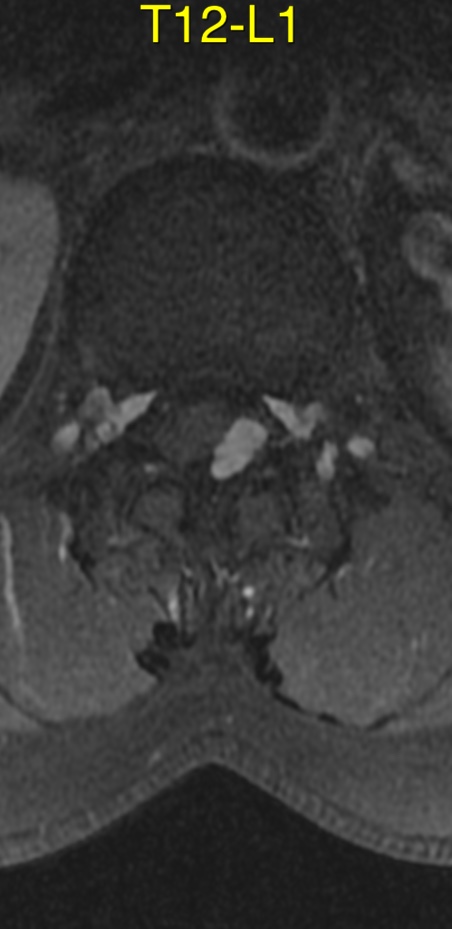
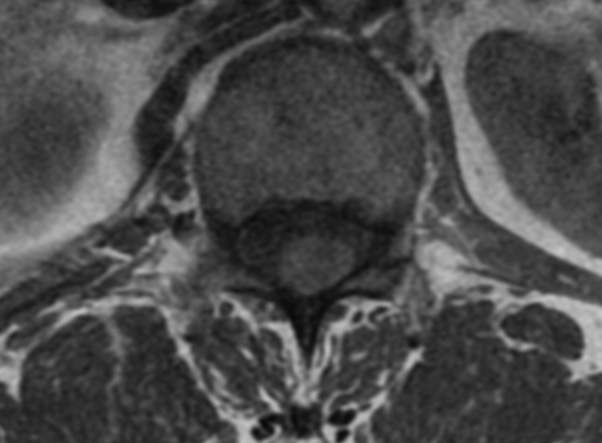
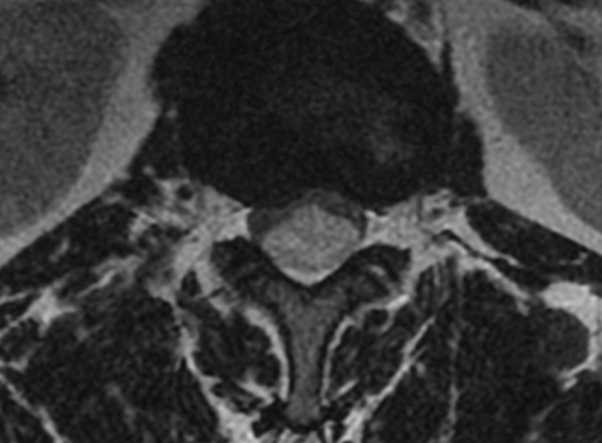
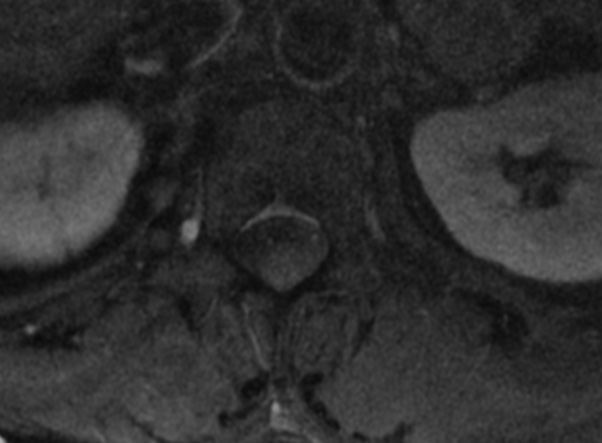
The MRI features consists of rounded cystic lesions arising from the medial aspect of degenerated facet joints filled with synovial fluid, usually smaller than 20 mm. They tend to course with lateral recess stenosis and present dense adhesions to dura and nerve roots.
The great majority of SCs arising from facet joints occur in the lumbar spine, L4/L5 being the most affected level. These lesions are seldom reported in the cervical spine and are even rarer in the thoracic spine.
They are thought to serve as drainage reservoirs for the excessive joint effusion in the setting of any arthropathy, escaping from its regular location through a one-way-valve mechanism into the area of least resistance.
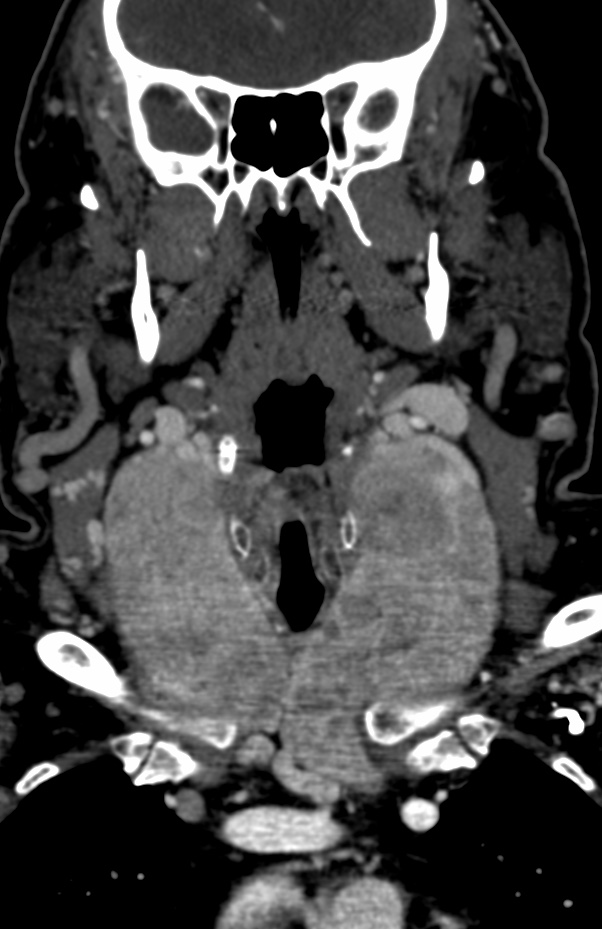
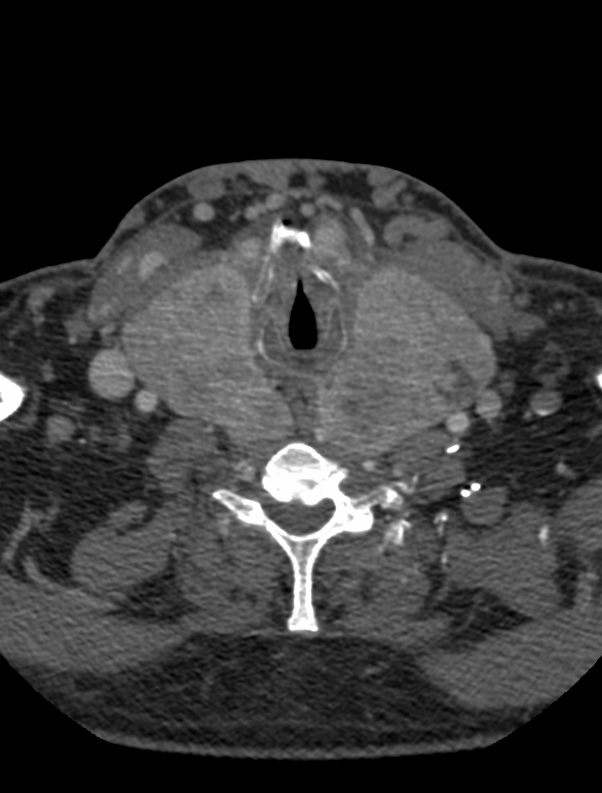
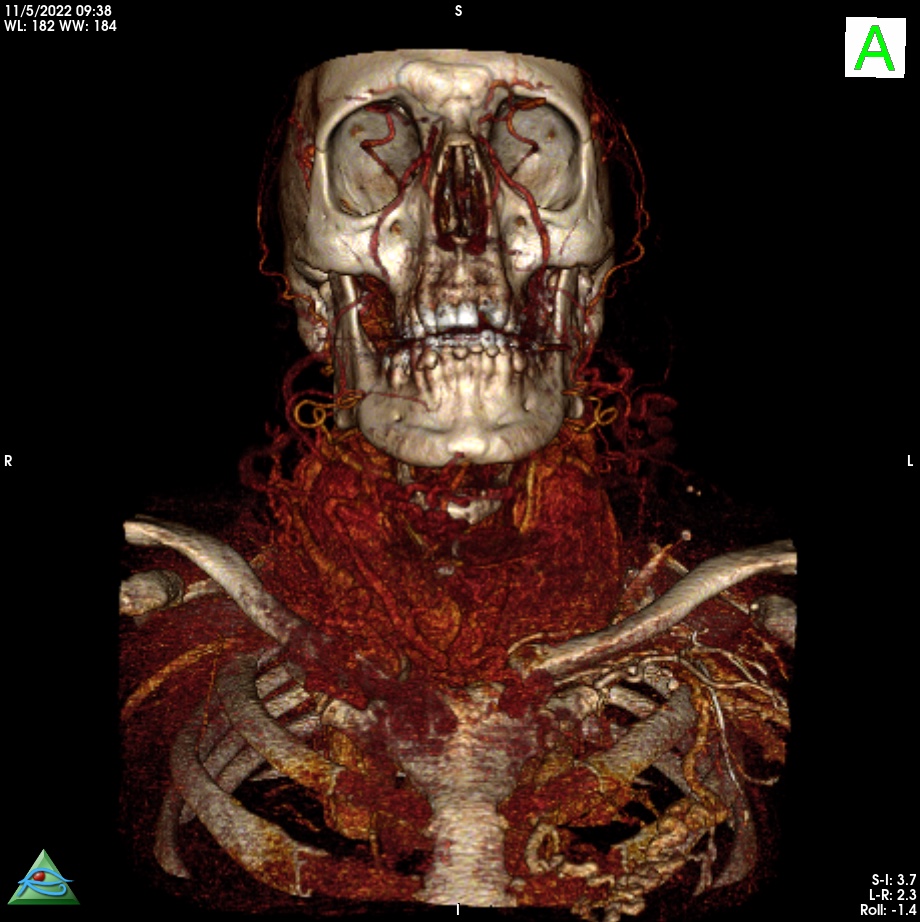
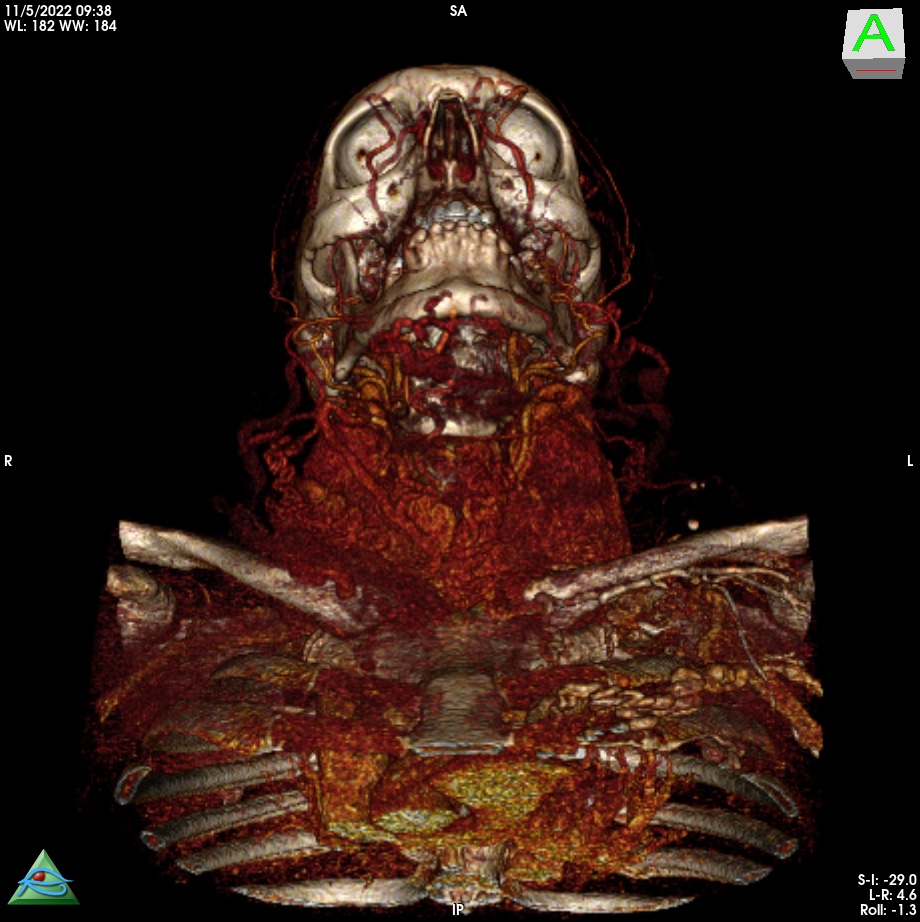
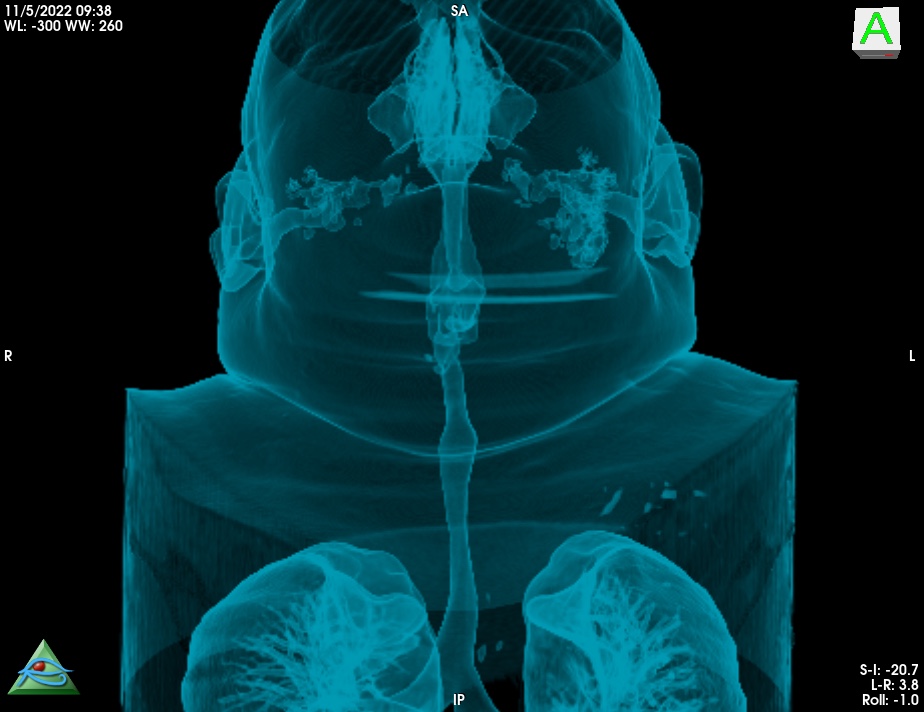
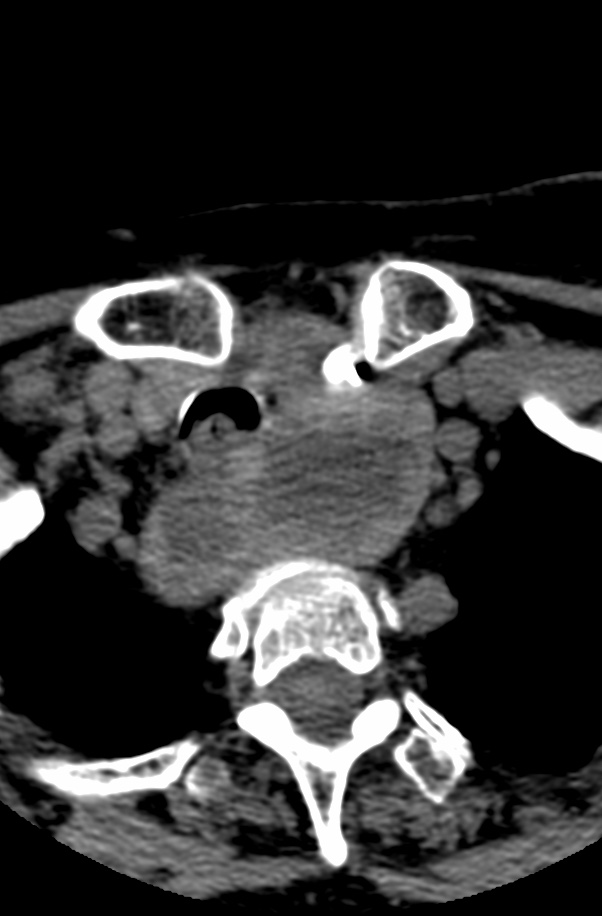
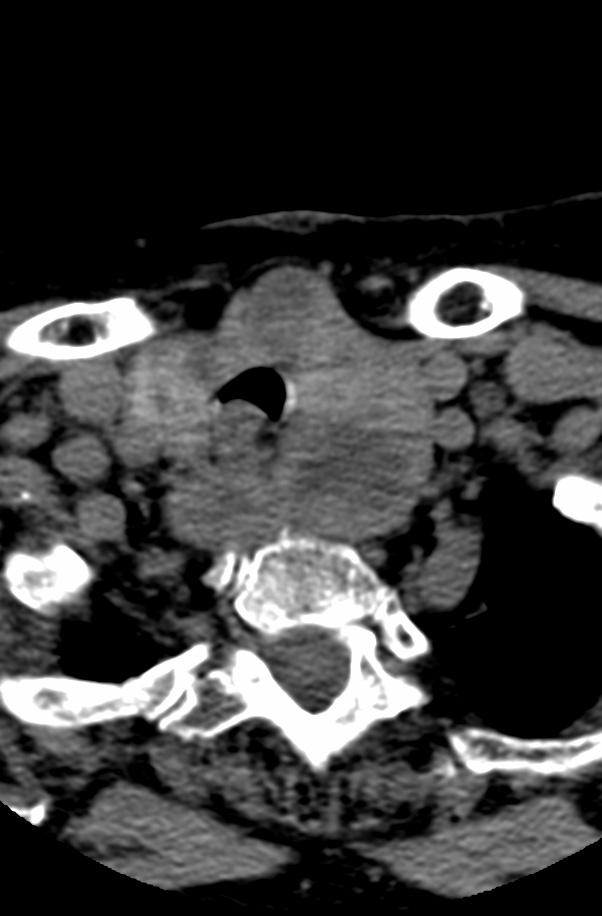
Thyroid goiters are estimated to occur in approximately 5% of the population worldwide . Most are in the neck, yet between 3% and 17% of these goiters extend into the thorax and are also called substernal, particularly when more than 50% of the mass is below the suprasternal notch . Intrathoracic goiters are usually in the anterior mediastinum. A small subset of 10-25% may be found in the posterior mediastinum Radiologic imaging is an important step in the workup of these patients because the surgical approach depends on the location and size of the intrathoracic goiter.
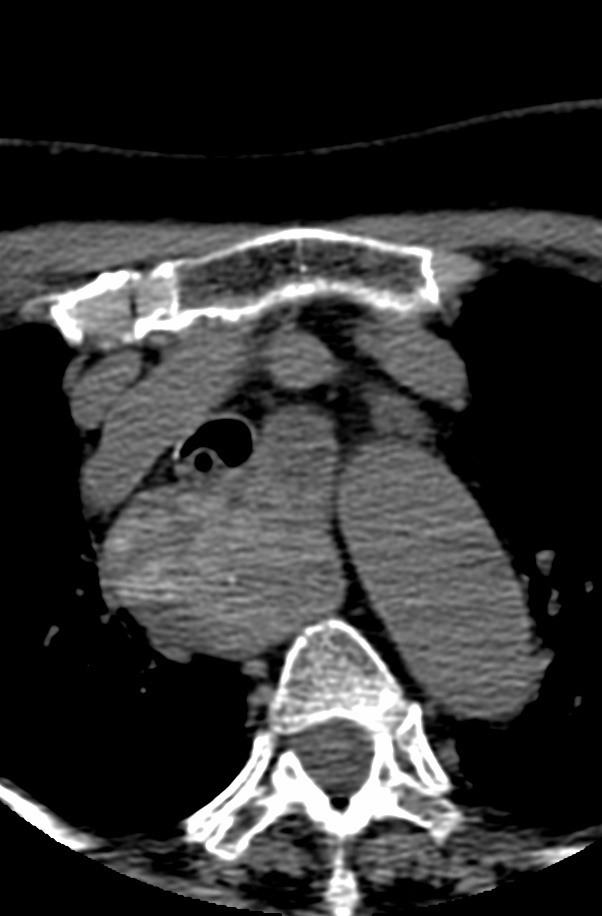
Anterior Versus Posterior: Most intrathoracic goiters lie anterior to the recurrent laryngeal nerve and anterolateral to the trachea. Goiters in the anterior mediastinum arise secondarily from the isthmus or the lower aspects of the thyroid lobes. As the mass grows inferiorly, the great vessels may be displaced laterally, framing the mass on chest radiography Posterior mediastinal goiters arise as secondary goiters from the posterolateral aspects of the thyroid gland and descend posterior to the great vessels. Most are right- sided because of anatomic barriers formed by the aortic arch and its branch vessels. Even goiters that originate from the left lobe are deflected to the right by the left innominate vein and left common carotid and subclavian arteries. The esophagus may be markedly displaced to the contralateral side and the trachea may be pushed anteriorly.
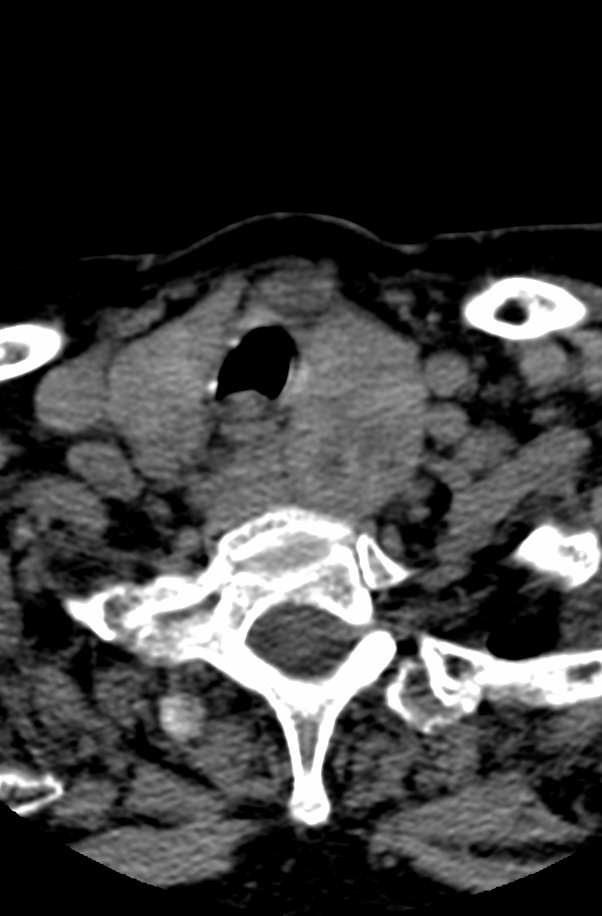
The goiter descends inferiorly along the fascial planes of the neck, following a path of least resistance into the superior mediastinum
case 2
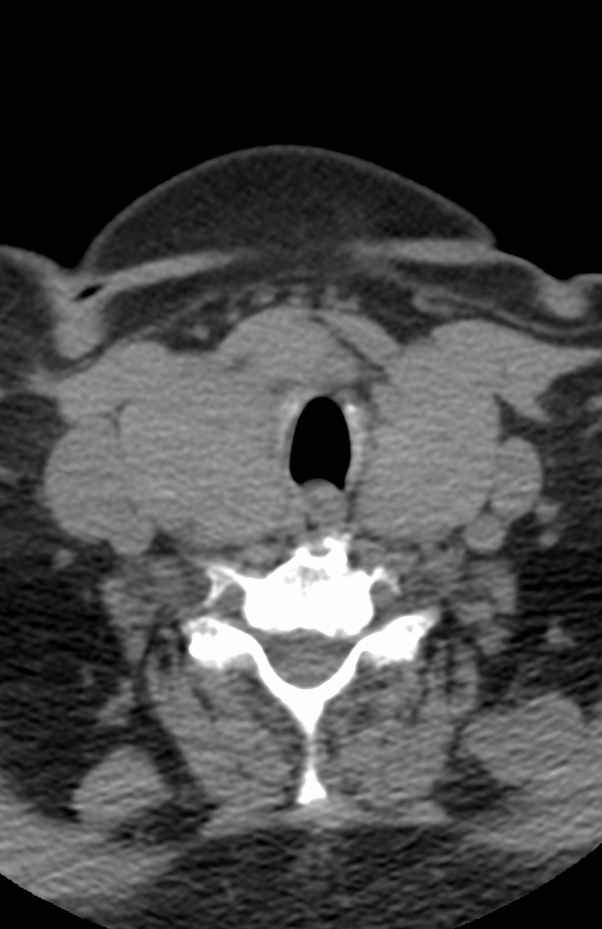
Although most patients are asymptomatic, stridor due to tracheal compression is the most common symptom . Findings include a sharply marginated mediastinal mass with punctate calcifications.
The differential diagnosis includes calcified lymph nodes. treated lymphoma. and a hemorrhagic primary mediastinal mass.
Myxopapillary ependymomas are highly vascular neoplasms characterized by abundant supporting fibrous connective tissue stroma, mucinous degeneration of this supporting stroma, and mucin secretion by the tumor cells.
Multiple tumors have been reported in 1 4%-43% of patients and may be due to dissemination of tumor in the spinal subarachnoid space. Certain sacral and presacral lesions behave aggressively and metastasize to the lymph nodes, lung, and bone . On the other hand, recurrence is rare following complete excision of well-circumscribed lesions.
Ependymomas of the brain frequently calcify, calcification is extremely unusual in spinal ependymoma.
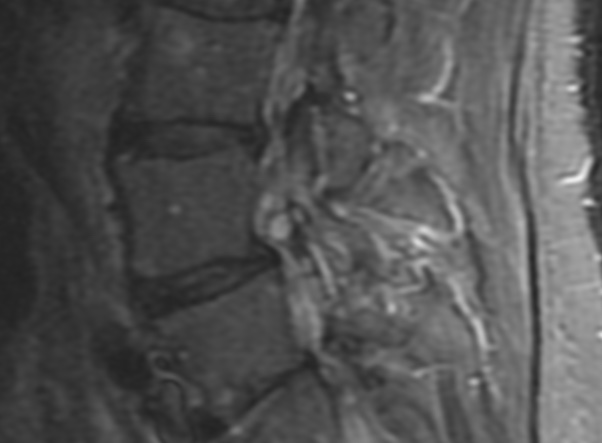
Bulky, obstructive lesions are associated with a high protein content of the CSF that may obscure differentiation of the tumor from the CSF. The signal intensity of the CSF can also be affected by subarachnoid hemorrhage. Almost all ependymomas enhance intensely after administration of contrast material. Contrast-enhanced imaging is useful in differentiating the tumor from the spinal cord, defining intratumoral cysts, and identifying intradural metastases.
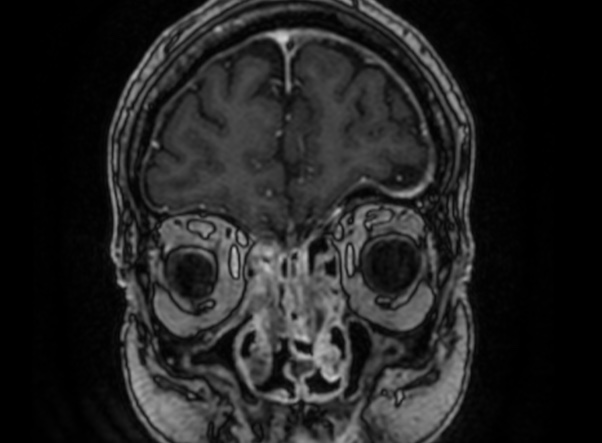
Idiopathic hypereosinophilic syndrome (HES) is a heterogeneous disorder characterized by prolonged eosinophilia without an identifiable cause, ultimately resulting in organ dysfunction.
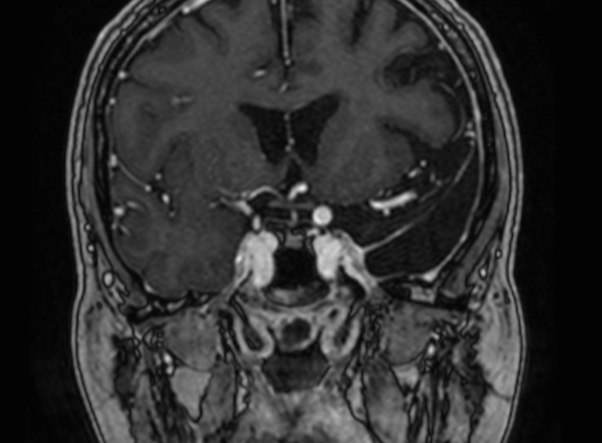
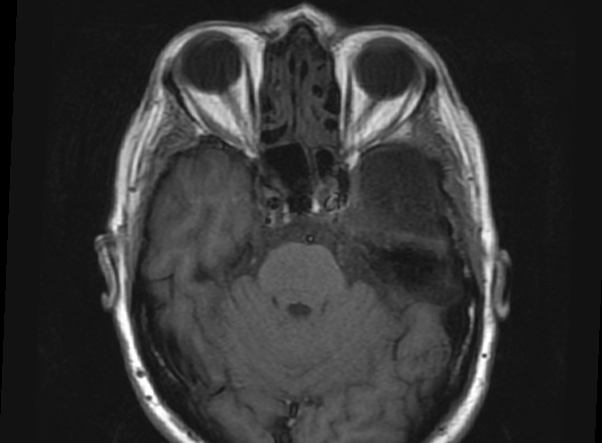
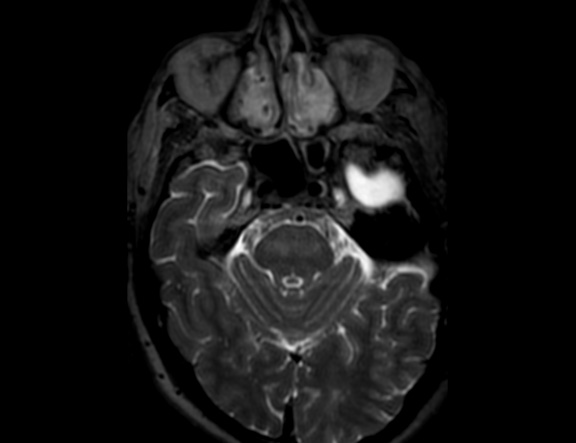
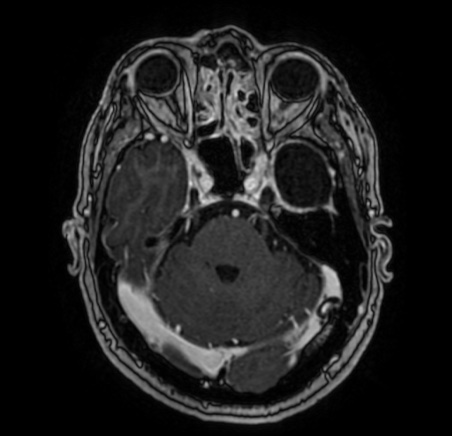
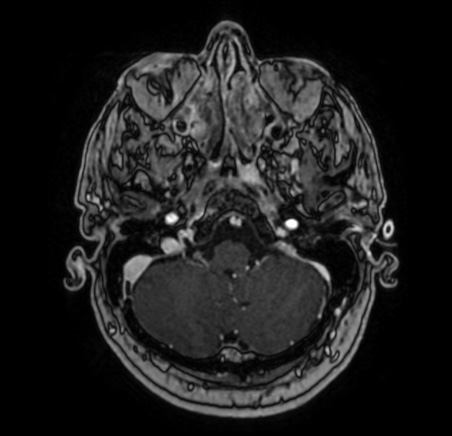
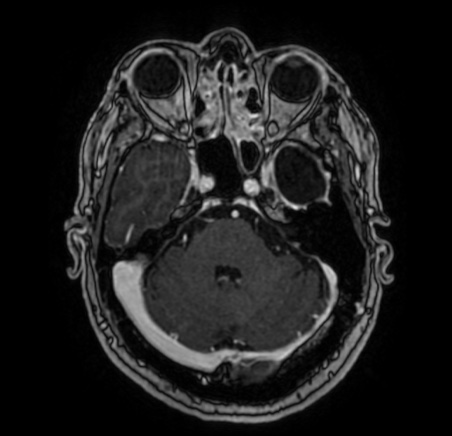
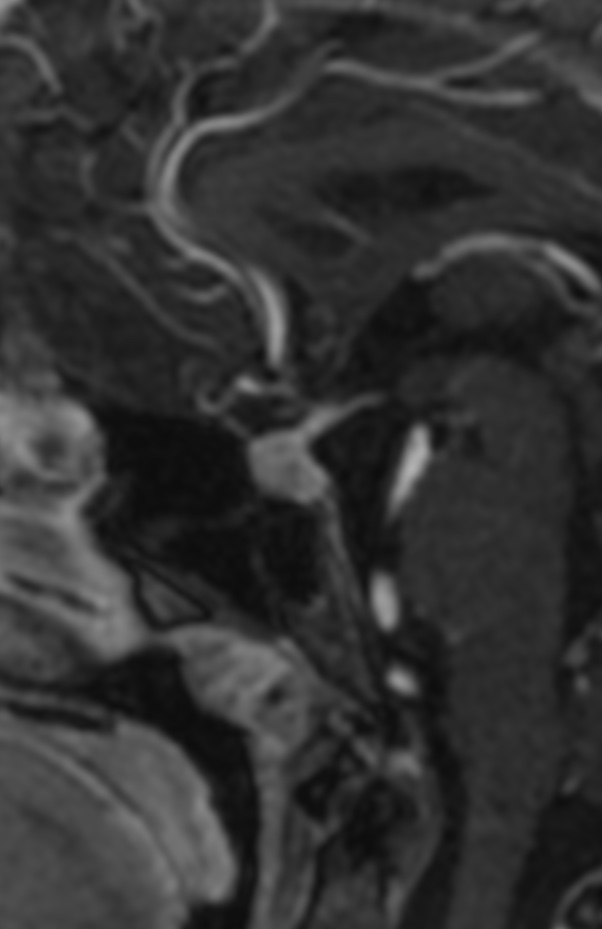
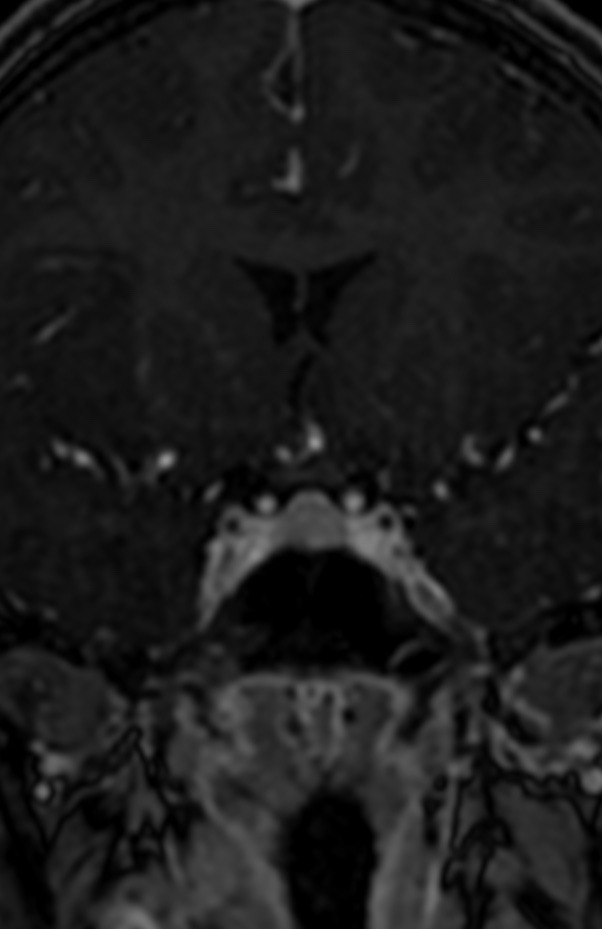
Idiopathic hypereosinophilic syndrome (HES) was first defined by Chusid et al in 1975 as unexplained eosinophilia of greater than 1500/μL present for longer than 6 months with evidence of organ injury related to the hypereosinophilia, such as cardiomyopathy, peripheral neuropathy, and encephalopathy. The heterogeneity of HES ranges from those patients with myeloproliferative features (splenomegaly, increased vitamin B12 levels, abnormal leukocyte alkaline phosphatase scores, and cytogenetic abnormalities) to those patients with benign courses (associated with increases in immunoglobulin E [IgE], angioedema, and corticosteroid-responsive eosinophilia). There is an unusual type of inflammatory pseudotumor (IPT) involving the skull base in a patient with HES who presented with multiple cranial nerve palsies.
It has a strong male preponderance, with a male-to-female ratio of 9:1, and most frequently involves the heart, lungs, nervous system, and skin.
In 1 series, 65% of patients with HES had neurologic involvement, and some reports have described recurrent optic neuritis as the presenting symptom of HES.
Three major types of neurologic involvement have been defined as follows: peripheral polyneuropathy, encephalopathy, and central nervous system (CNS) thromboemboli. Peripheral polyneuropathy is most common, occurring in approximately 50% of patients with HES, and may manifest as a sensory neuropathy, mononeuritis multiplex, radiculopathy, or muscle atrophy caused by denervation.
Patients with encephalopathy have memory loss, confusion, ataxia, incoordination, weakness, and upper motor neuron signs including increased muscle tone, deep tendon reflexes, and a positive Babinski reflex. Seizures, intracranial hemorrhages, dementia, and organic psychoses occur less frequently. Eosinophilic meningitis occurs uncommonly. The pathogenesis of both the encephalopathy and peripheral neuropathy of HES remains unknown. Possible mechanisms include direct damage from the infiltration of eosinophils and other inflammatory cells and injury from a toxin originating within eosinophils.
Embolic disease to the CNS may be caused by intracardiac thrombus formation secondary to eosinophilic infiltration resulting in endomyocardial fibrosis and thrombus formation. However, thromboemboli may also occur without demonstrable cardiac disease and can be the presenting manifestation of HES. In these cases, it has been postulated that thrombosis within the vessels of the CNS may be the underlying mechanism.
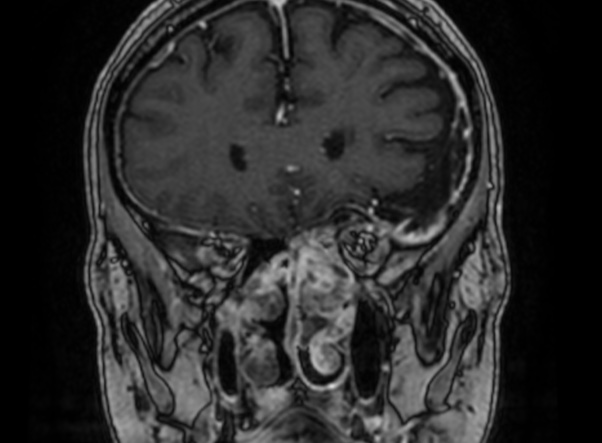
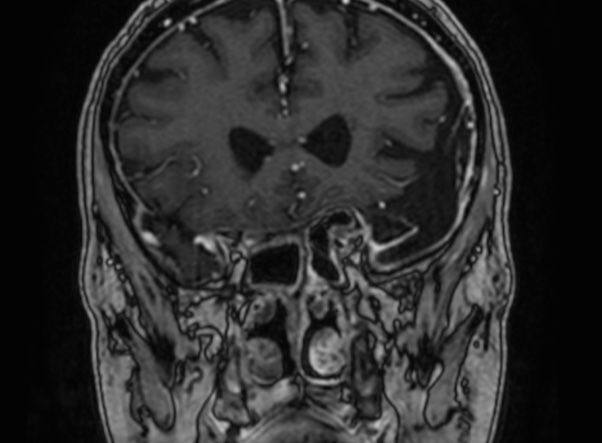
IPT is a clinicopathologic term used to describe a reactive inflammatory and nonneoplastic process. In the literature, “pseudotumor” has been given many different names, some of which are plasma cell granuloma, plasmacytoma, inflammatory myofibroblastic tumor proliferation, and histiocytoma. IPT has been described most often in the lung and orbit, with other systemic sites somewhat less frequently. Involvement of the CNS parenchyma by IPT is rare. The lesions occur throughout the brain parenchyma and meninges, without restriction to a particular area. IPT can both clinically and radiologically mimic a malignant process.
The differential diagnostic considerations of a mass in the cavernous sinus with dural enhancement include meningioma, lymphoma, neurosarcoidosis, infection, and amyloidosis.
Reference:
American Journal of Neuroradiology May 2007, 28 (5) 971-973;
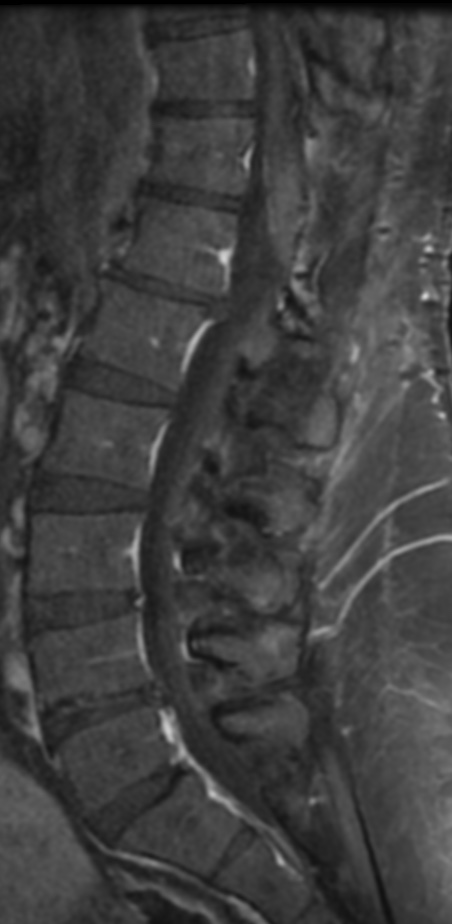
Myxopapillary ependymoma is a distinct subtype of spinal cord ependymomas that has a predilection for the lumbosacral region.
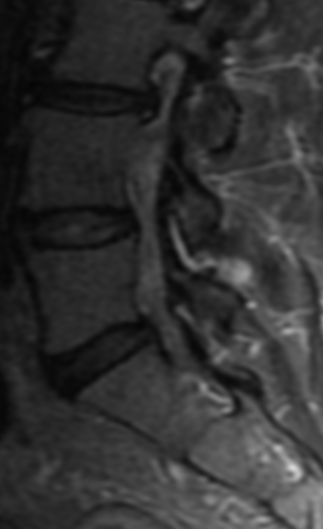
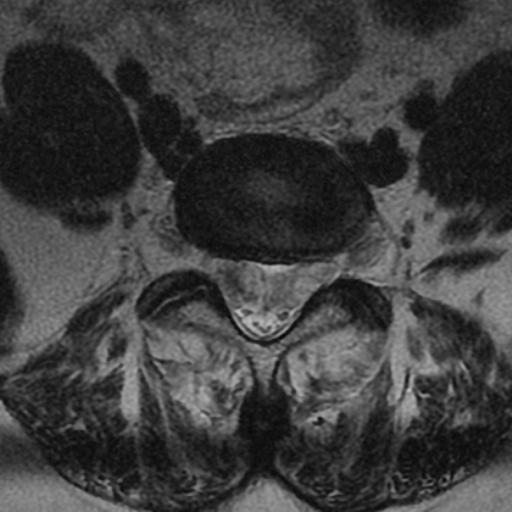
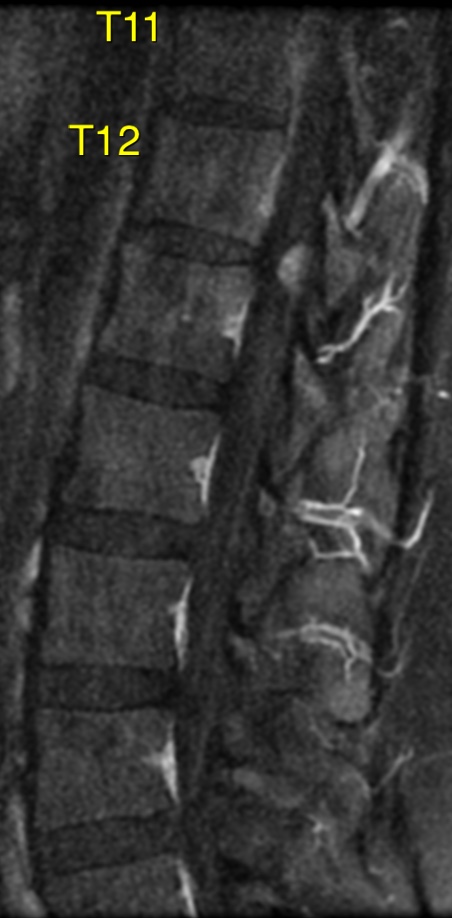
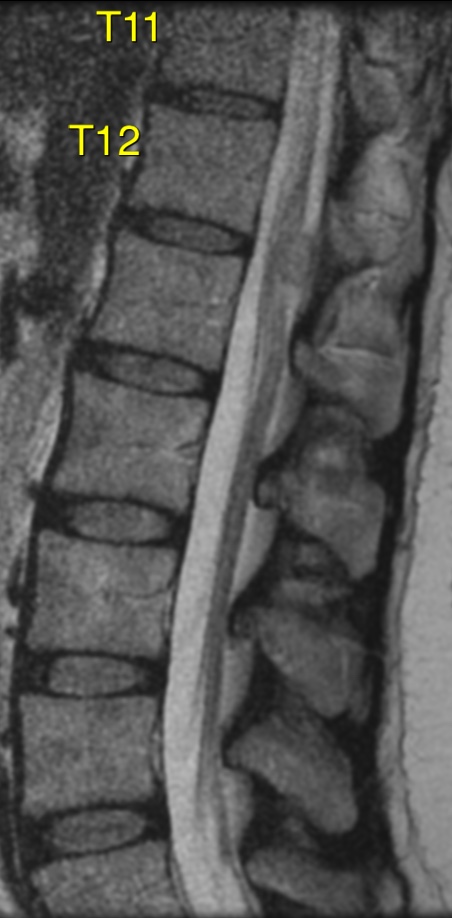
Magnetic resonance imaging is helpful in identifying the extent of the tumor and its relationship to intraspinal structures. It also allows for visualization of the cauda equina both above and below the tumor and will identify drop metastases in the subarachnoid space. Such information is useful in preoperative surgical planning. Magnetic resonance imaging findings in myxopapillary ependymomas are nonspecific.
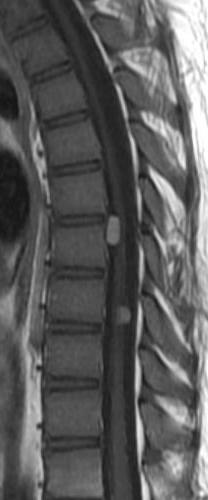
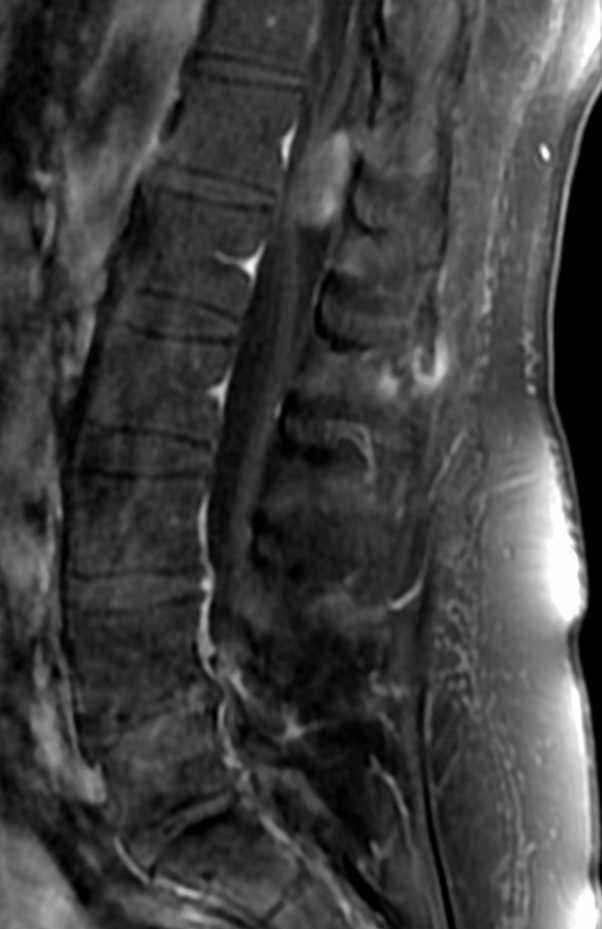
On magnetic resonance imaging, the lesion is iso- to hypointense on T1 and hyperintense on T2. Owing to their mucin content, the signal is hyperintense in myxopapillary ependymoma. Moreover, the tumor is heterogeneous after gadolinium injection. Hemorrhage and cyst formations are common features that contribute to signal inhomogeneity.
However, these tumors do contain certain features that help suggest the diagnosis. These features include:
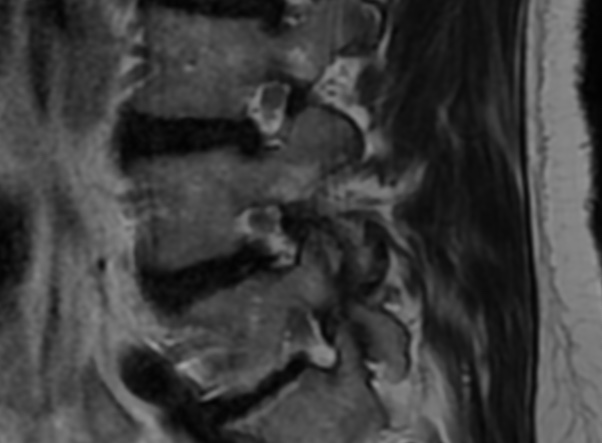
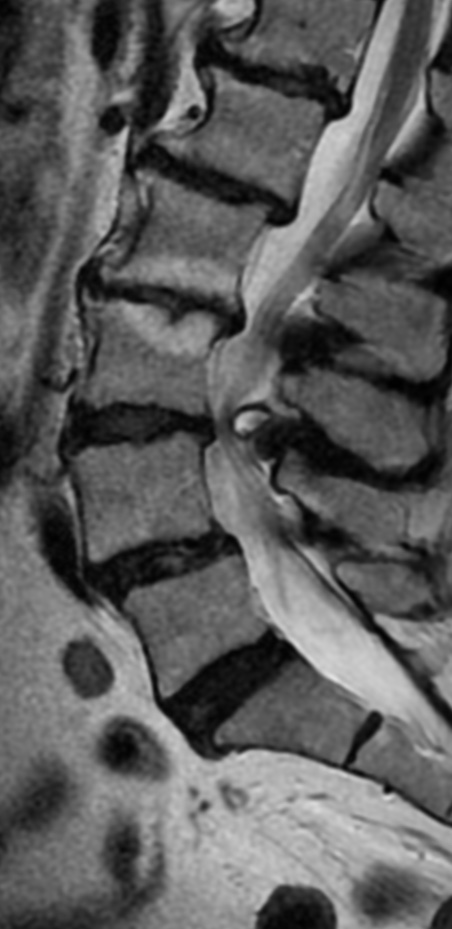
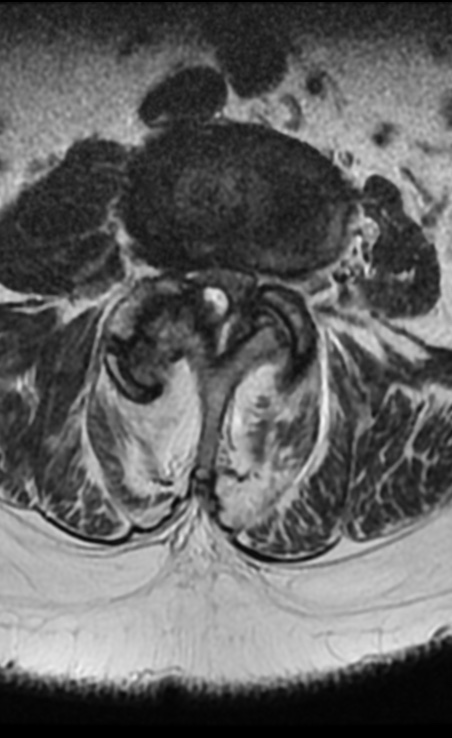
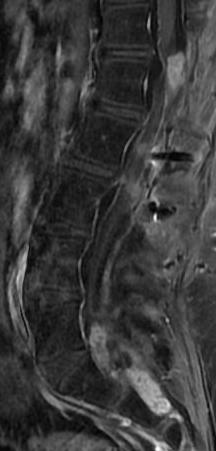
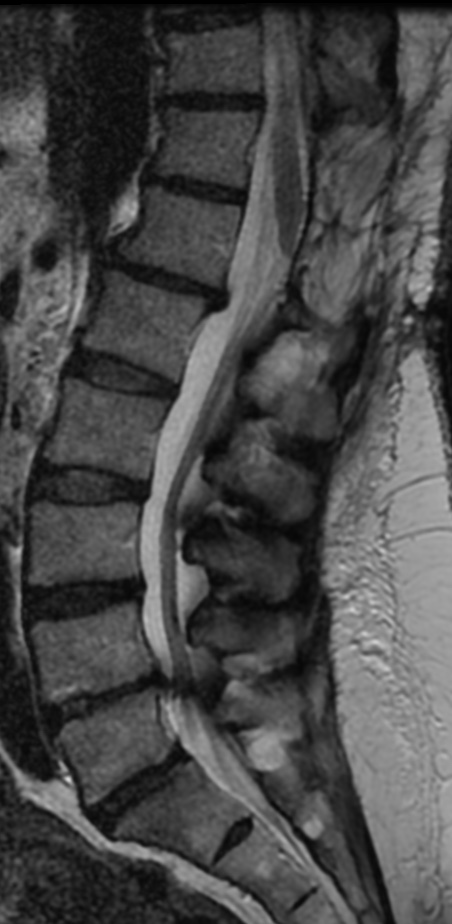
An intradural extramedullary thoracolumbar mass
The tumor extends for several vertebral levels in the lumbar and sacral canal.
It is hypointense to isointense on T1-weighted images.
It is hyperintense on T2 weighted images.
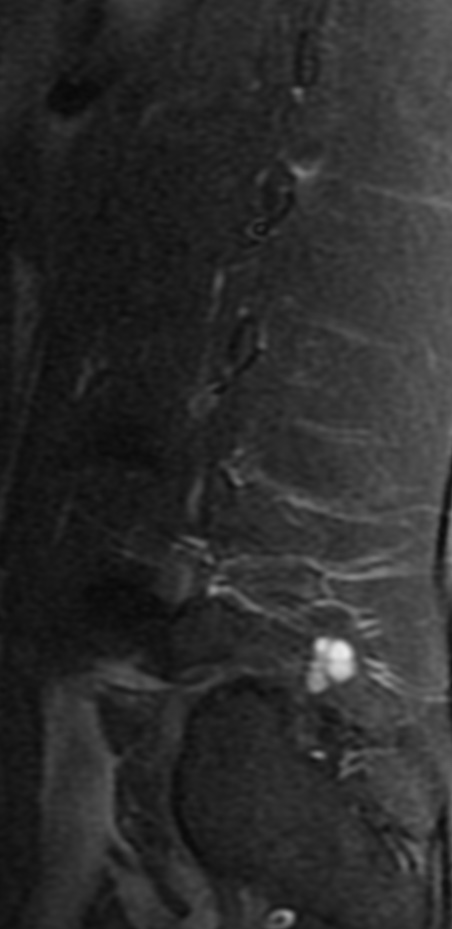
There will be an intense, homogeneous enhancement after the administration of contrast.
There will usually be a region of slightly lower intensity at tumor margin on T2-weighted sequences.
Cystic rostral or caudal degeneration exists in 50% of cases.
Ependymomas of the brain frequently calcify, calcification is extremely unusual in spinal ependymoma.
The differential diagnoses of filum terminale and small conus myxopapillary ependymomas include:
Fibrous meningioma:The fibrillary variant of myxopapillary ependymomas may be confused with fibrous meningioma
Schwannoma: The fibrillary variant of myxopapillary ependymomas may be confused with schwannoma
It represents 13% of all spinal ependymomas and accounts for 90% of all tumors in the conus medullaris. Myxopapillary ependymoma is a benign and slow-growing neoplasm.
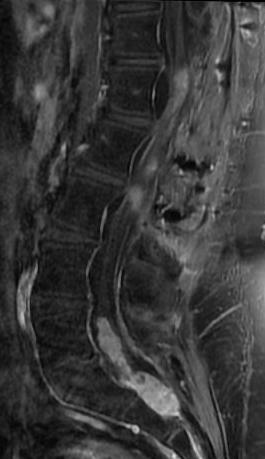
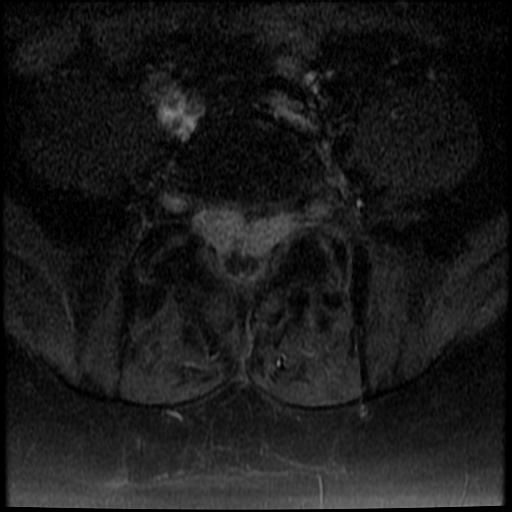
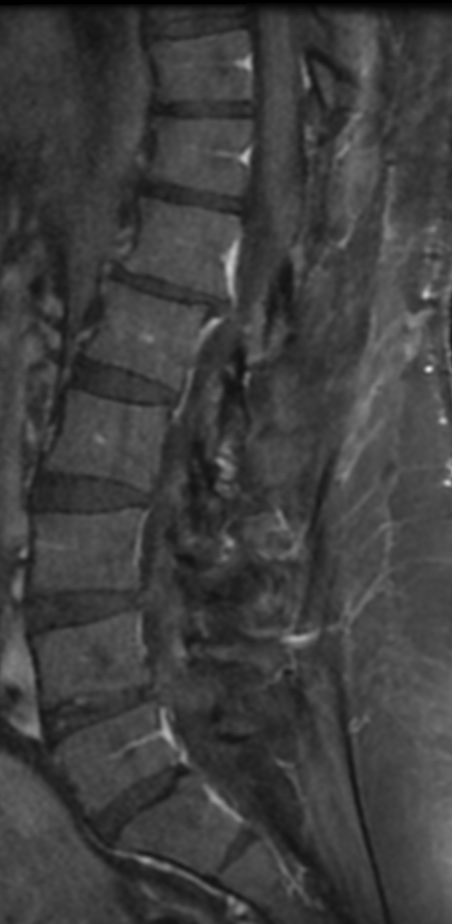
28f. Case 2. Despite the good results with surgery, tumor recurrence and dissemination may occur. Local recurrence and metastases have been related to the clinical history of less than 1 year, the extent of resection, atypical histology, and lesions extending into the substance of the spinal cord. Myxopapillary ependymomas are considered benign tumors of the central nervous system with long-term survival rates and a tendency for local recurrence. However, an aggressive course has occasionally been described, leading to cerebrospinal fluid dissemination and even systemic metastases.
Myxopapillary ependymoma arises from the ependymal glia of the filum terminale. No risk factors for the development of this tumor have been described. Extradural myxopapillary ependymomas are thought to arise from the coccygeal medullary vestige or the extradural remnants of the filum terminale.
Myxopapillary ependymomas account for 1% to 5% of all spinal neoplasms and approximately 13% of all spinal ependymomas. In the American population, their incidence was 1.00 per million person-years. The age at onset varies between 30 and 50 years (mean age, 35 years). The most common location of myxopapillary ependymoma is the lumbosacral spine segment, mainly in the conus medullaris and cauda equina regions. Other rare locations include the cerebral ventricles and the brain.
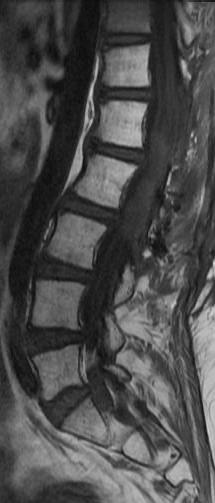
Post Surg. Controlcontrolcontrolcase 3. 34F
Early detection and treatment of patients affected by myxopapillary ependymomas are crucial to achieving optimal patient outcomes. The best treatment modality for myxopapillary ependymoma is complete surgical resection, which is associated with a complete resolution for the majority of patients. Surgery should be performed early so as to guarantee better postoperative outcomes. Complete resection of this tumor may be hazardous, principally if the tumor involves the conus medullaris or is interlaced with the nerve roots of the cauda equina. Surgeons must be very careful since nerve roots may also penetrate directly through the tumor.
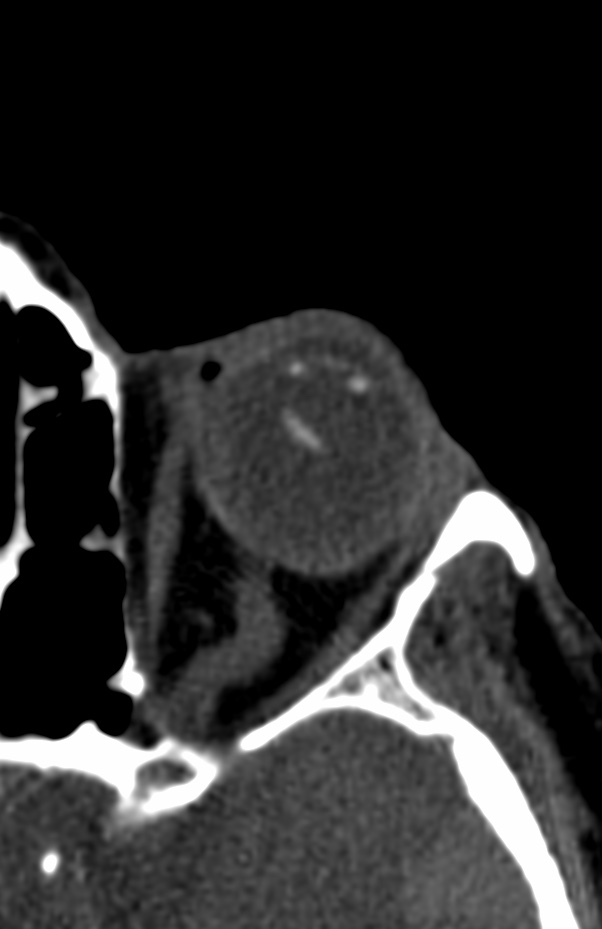
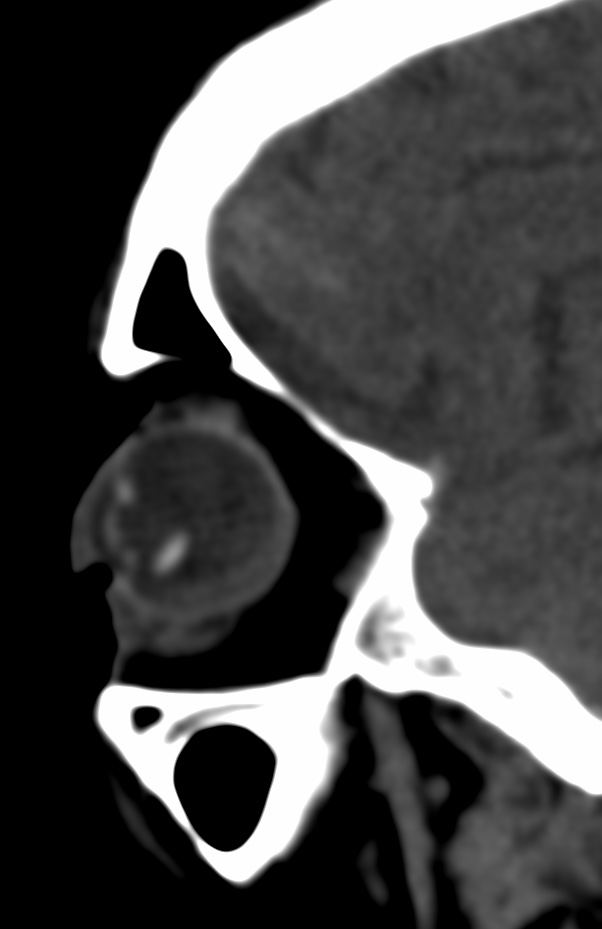
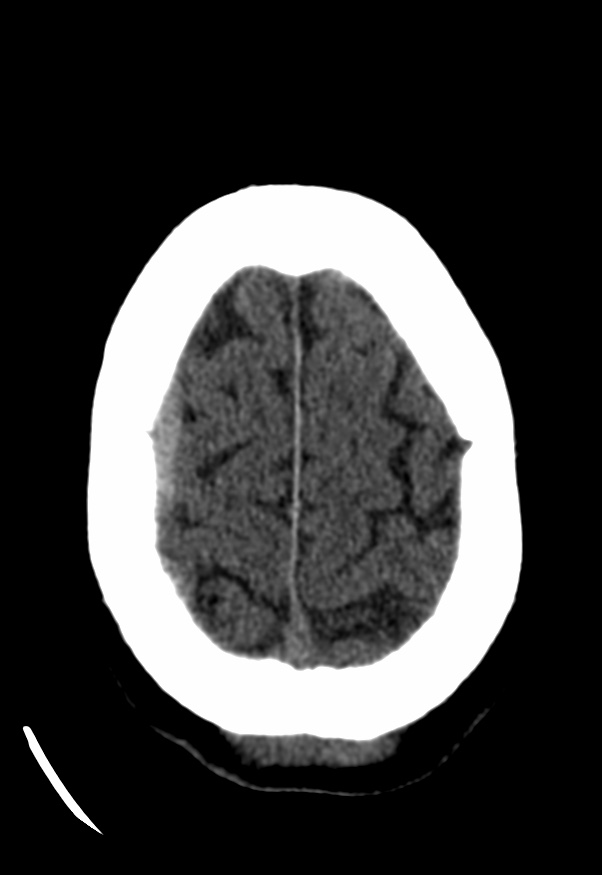
Blunt trauma may cause sudden compressive deformation of the globe causing transient shortening of the eye in the anterior-posterior direction displacing the cornea and anterior sclera posteriorly. This causes a compensatory expansion of the globe in the equatorial plane, which can stretch or break the zonules.
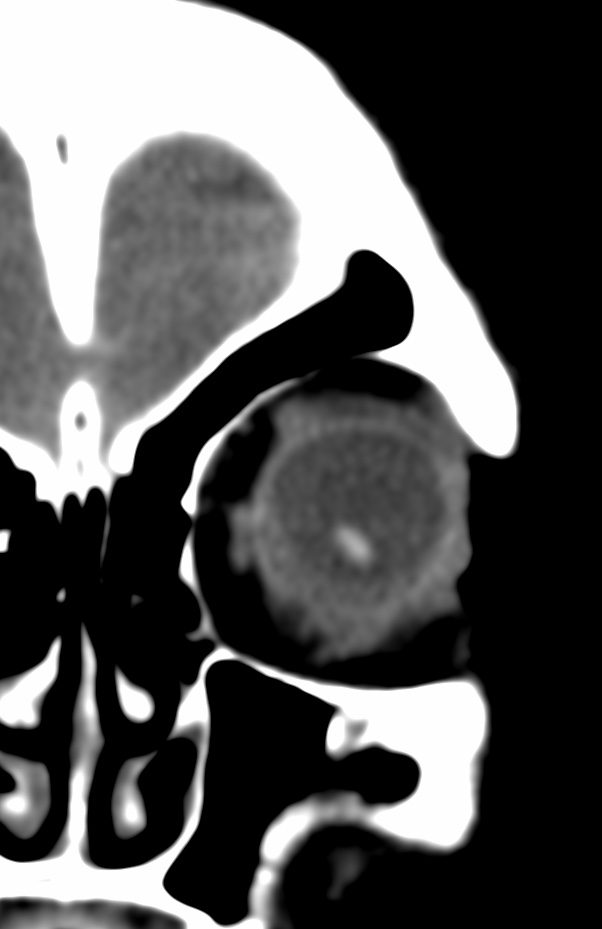
Partial or complete disruption of zonular fibers leads to subluxation or dislocation of the lens into the posterior chamber.
The differentiation between complete and partial zonular tear is essential as it can alter management.
Radiologic imaging is not a substitute for a thorough direct ophthalmologic examination, it may be of occasional help in cases where a direct examination is not immediately possible which may be the case in a noncooperative patient (inebriated or posttraumatic) or due to extensive soft tissue injury. Thus, knowledge of this condition is essential and meticulous evaluation of the orbit and its contents is imperative in all routine CT scan of the heads, not only for medicolegal documentation purposes but also for prompt recognition and intervention.
Beside trauma, lens dislocation is seen in hereditary disorder like congenital aniridia, congenital glaucoma, cystathionine b-synthase deficiency, Ehlers-Danlos syndrome, focal dermal hypoplasia, homocystinuria, Kniest dysplasia, Marfan’s syndrome, molybdenum cofactor deficiency, sulfite oxidase deficiency, Weill-Marchesani syndrome.
Direction of dislocation dictates management. Anterior lens dislocation requires lens removal. Refractory glaucoma, persistent uveitis, or corneal damage are indications for urgent or emergent intervention. Posterior dislocation may be managed conservatively by correction with aphakic contact lenses. Lens removal in posterior dislocations should be considered in patients that do not tolerate correction, suffer symptoms despite correction, or develop glaucoma or persistent uveitis. If the patient undergoes surgery for another posterior chamber pathology lens removal may also be considered.
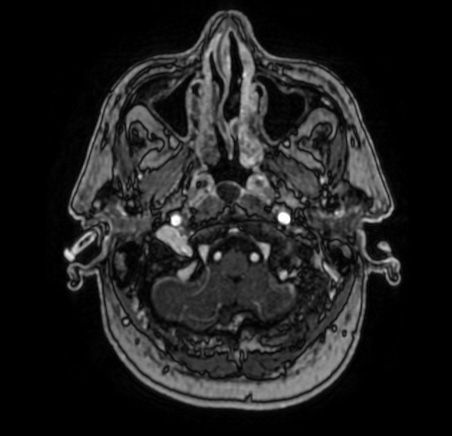
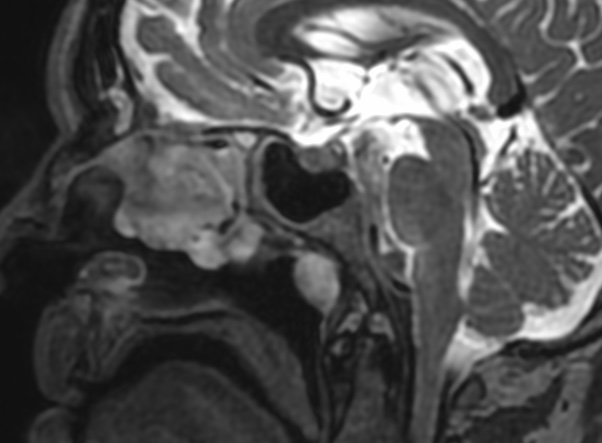
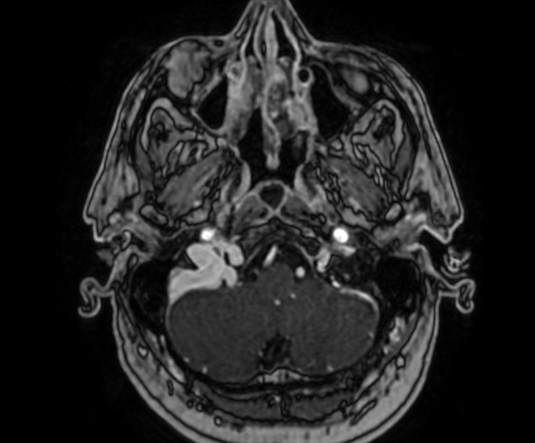
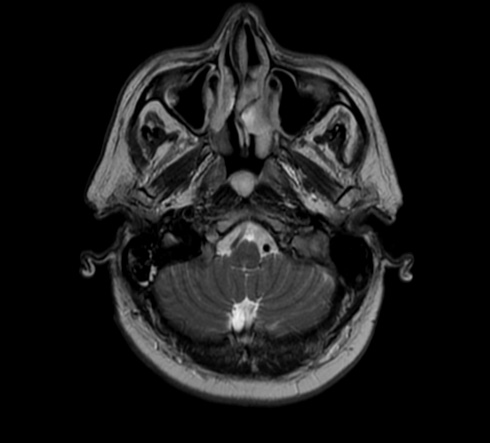
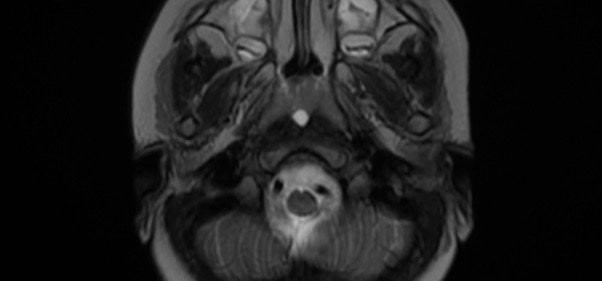
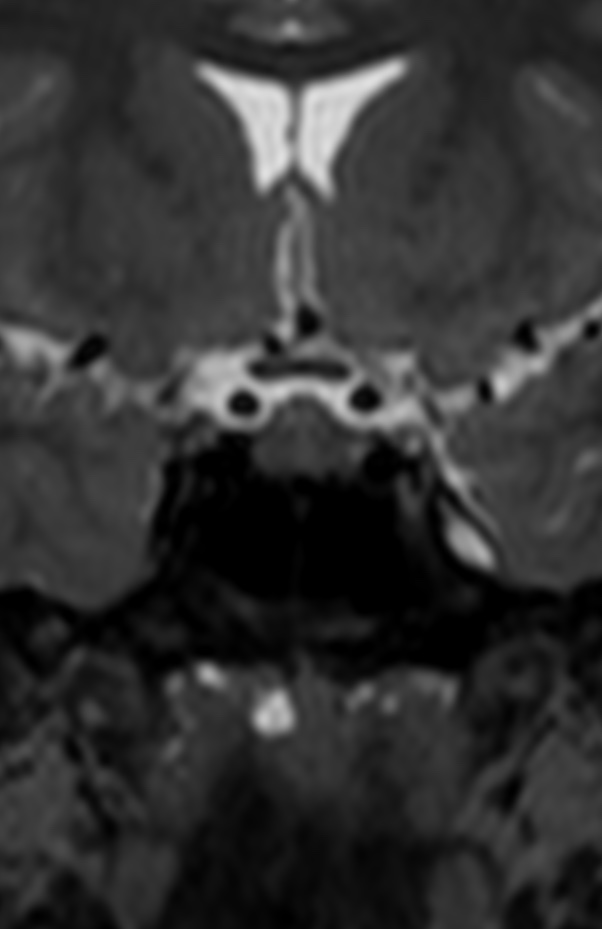
The Thornwaldt cyst is a benign cystic lesion that develops in the posterior medial wall of the nasopharynx; its incidence is 4% on autopsy samples, however an incidence of 0.2 to 5% has been observed on routine brain and cervical MRI.
The etiopathogeny remains controversial, some assume that it is a relic of the notochord (embryonic tissues from which vertebrae are formed), while others evoke an iatrogenic occlusion of normal structure after adenoidectomy or chronic inflammation
The Tornwaldt cyst is most often asymptomatic; however, an increase in its volume or inflammation may cause occipital headache, nasal obstruction with persistent discharge, bad breath, cervical myalgia, eustachian tube dysfunction, and sometimes infections of the middle ear
MRI remains the reference examination to identify this lesion, with a hypo or a T1 signal (depending on the protein content of the cyst) and a hypersignal T2
The main differential diagnoses are: Rathke’s pocket cyst, meningocele, meningoencephalocele and necrotic nasopharyngeal tumors
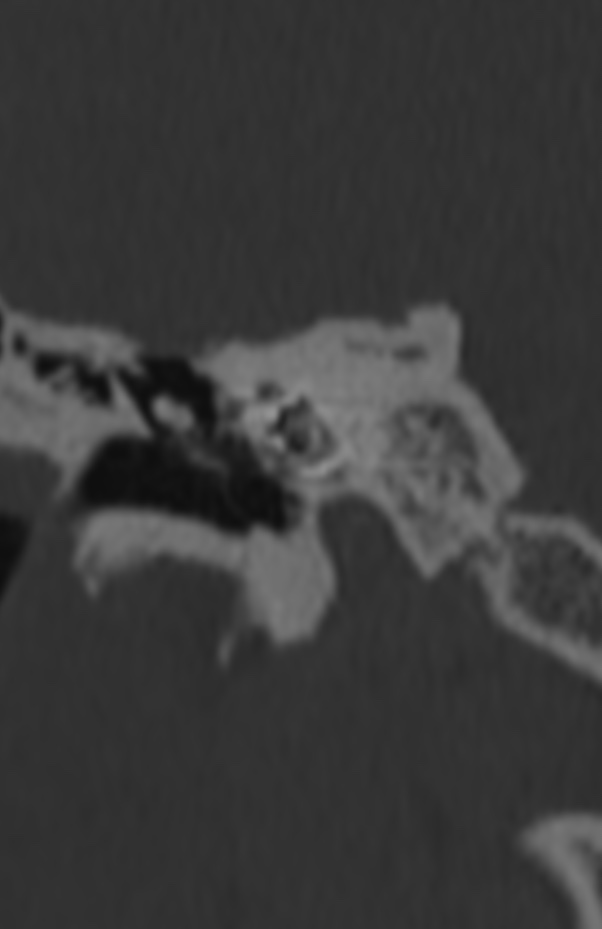
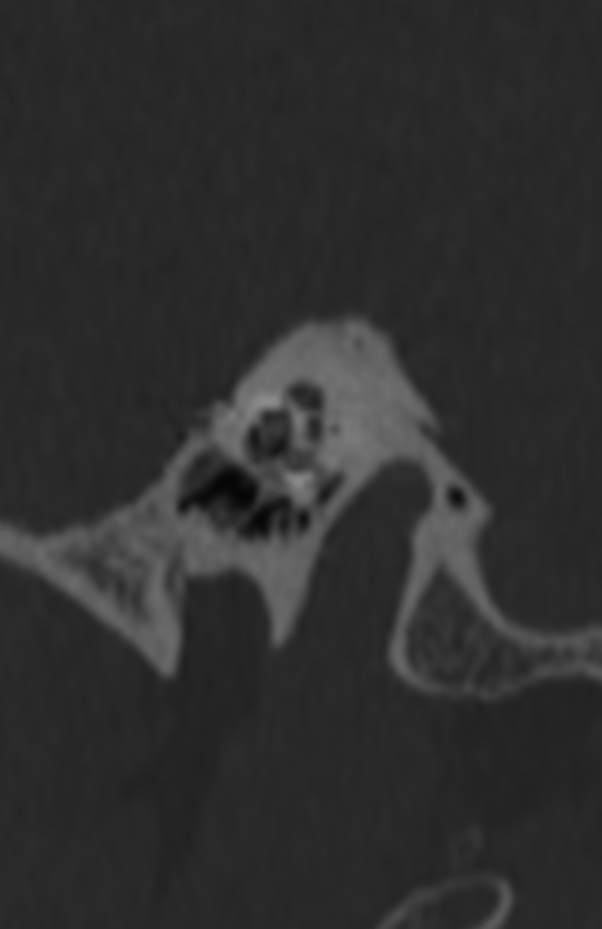
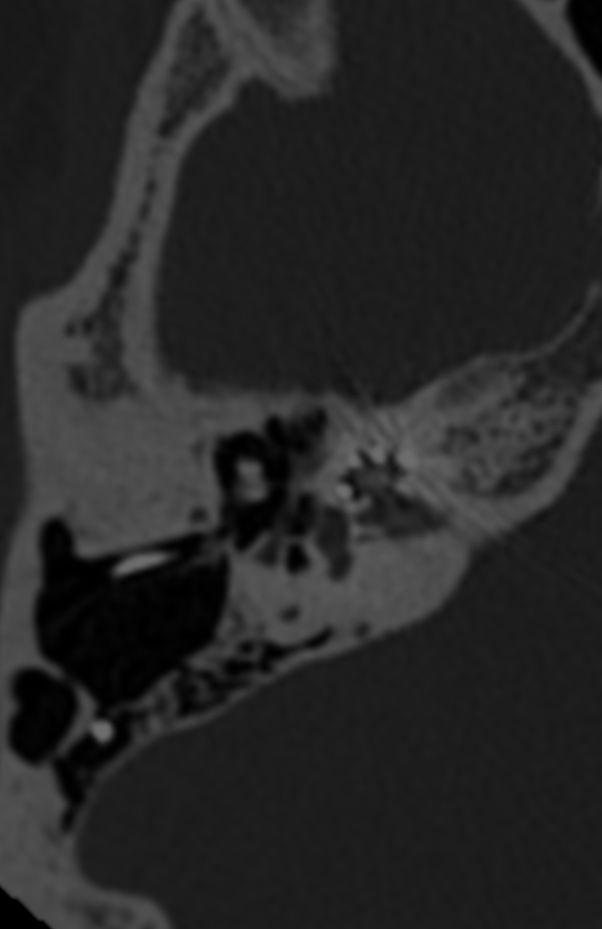
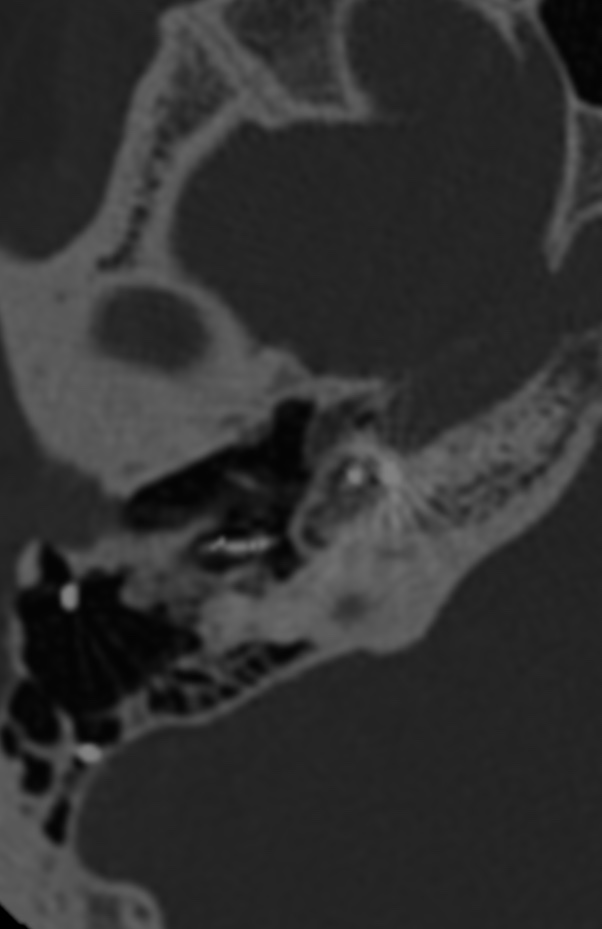
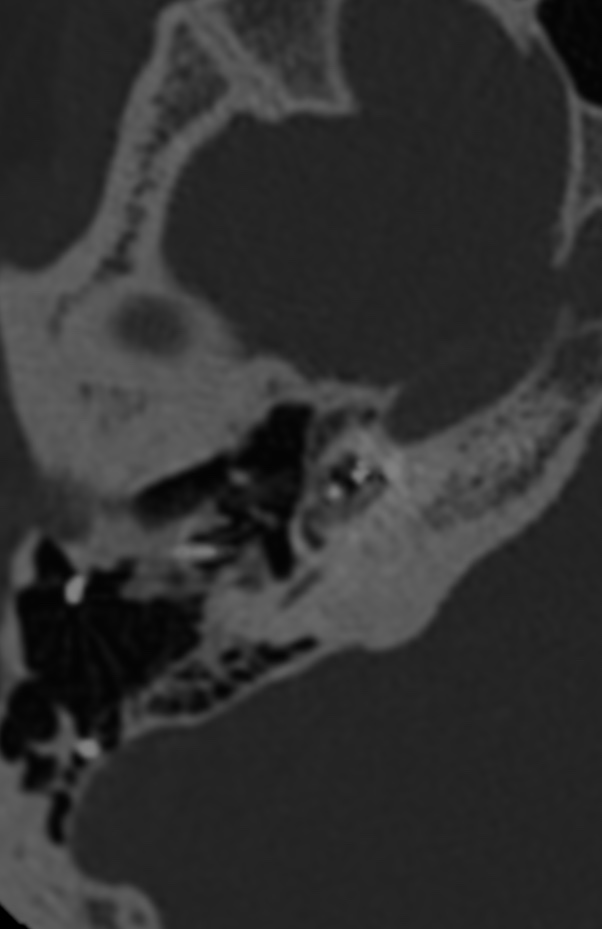
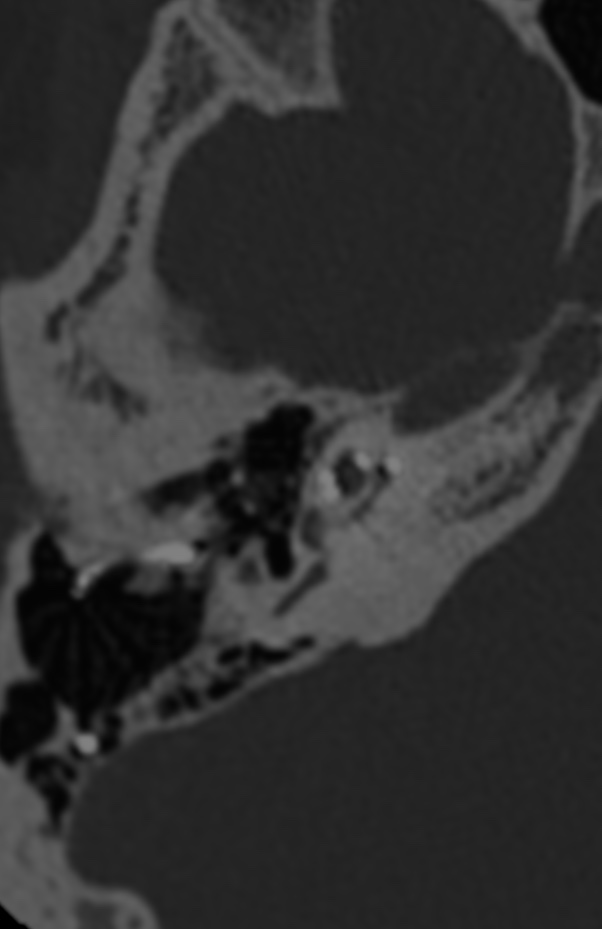
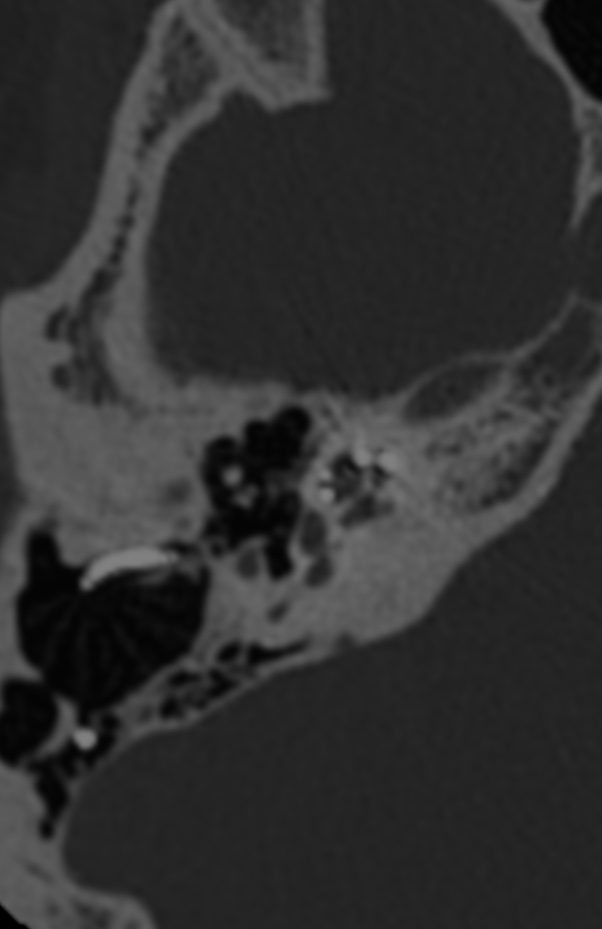
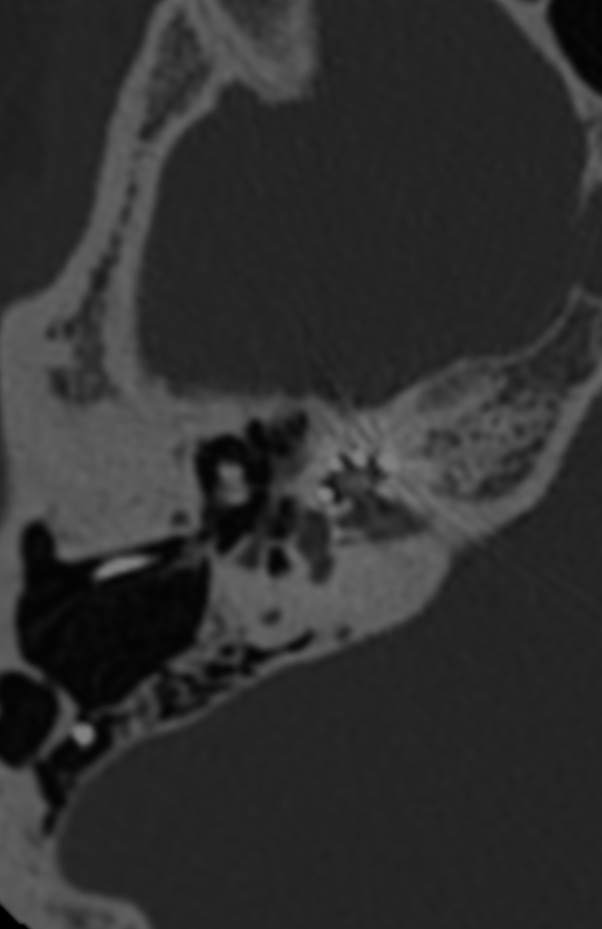
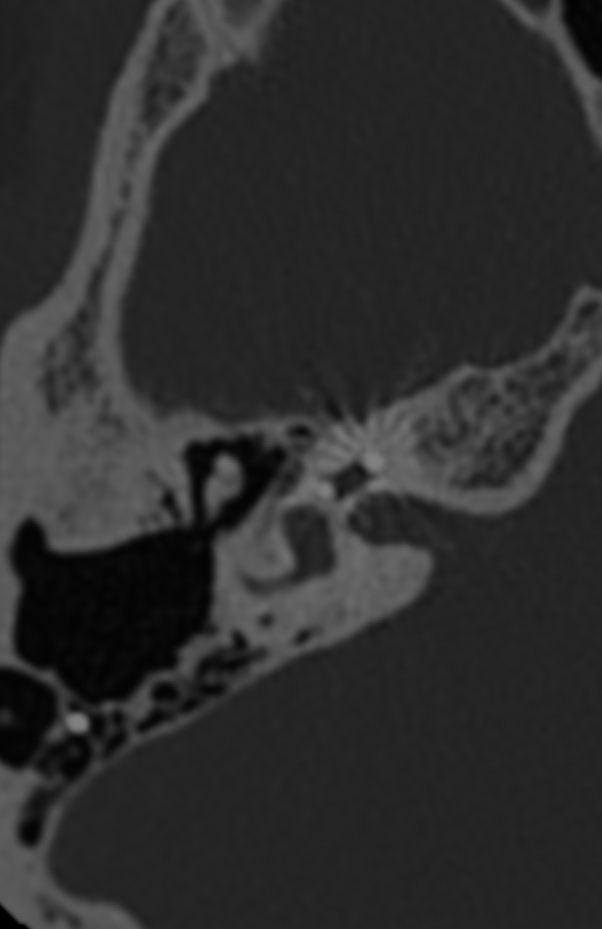
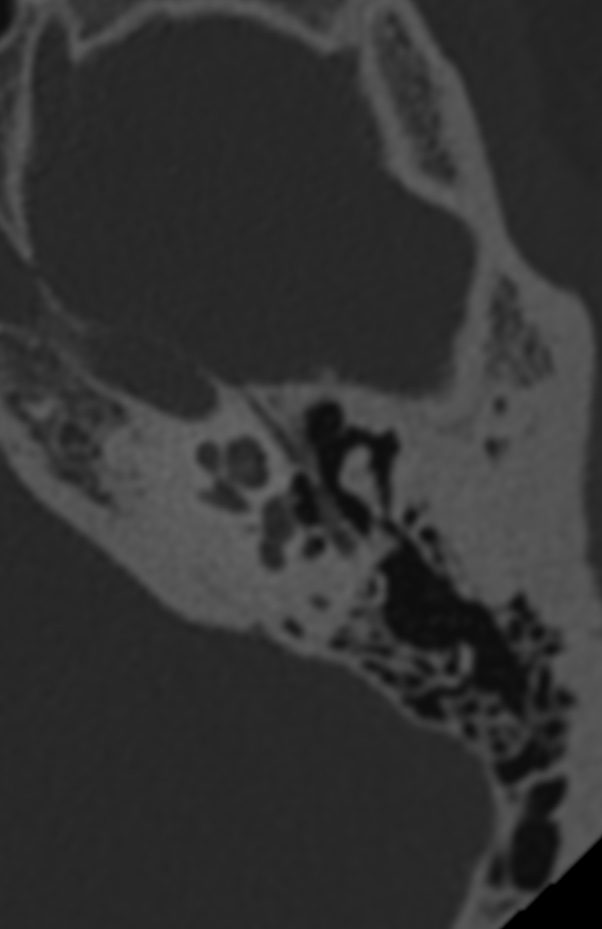
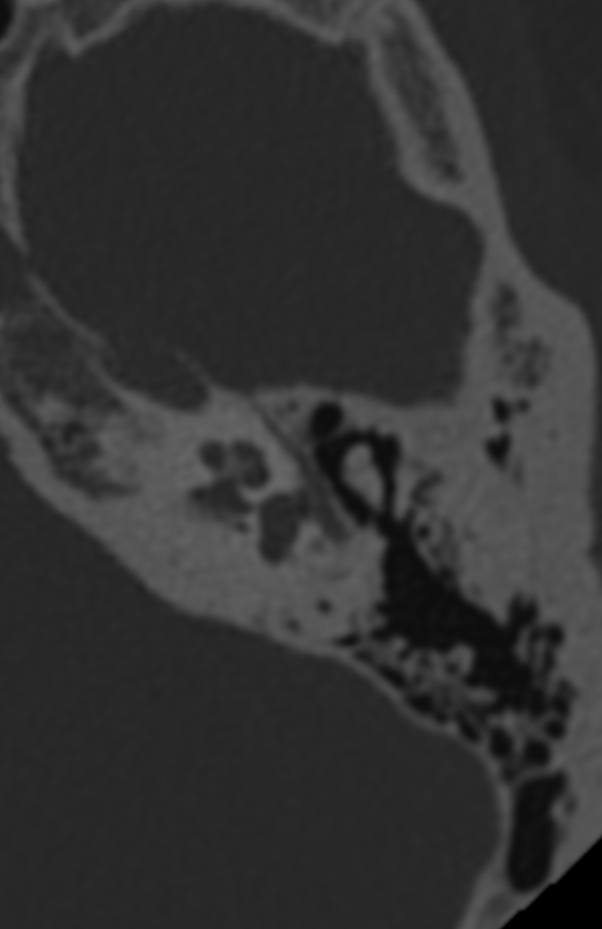
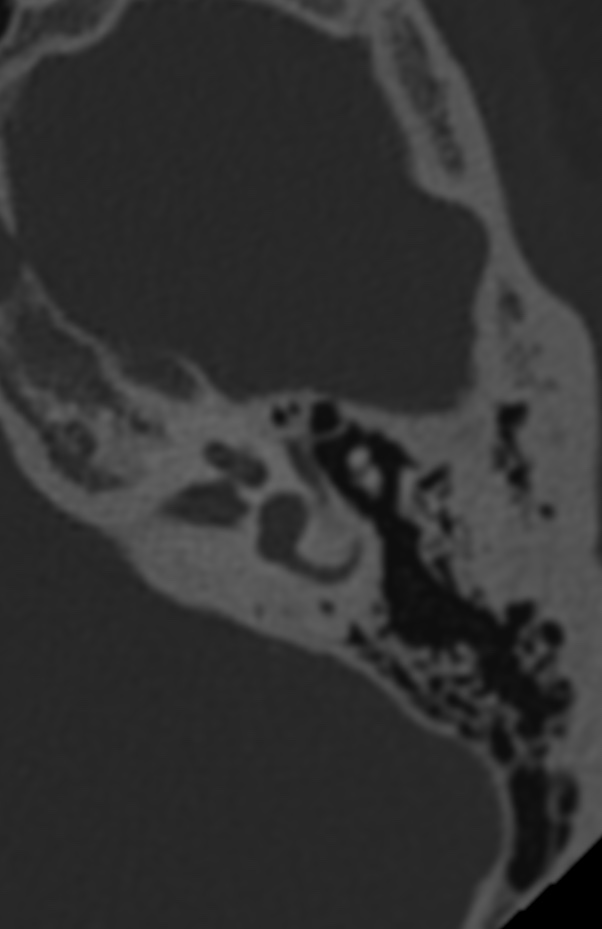
A cochlear implant is a neuroprosthetic device that forms an effective solution for patients with severe-to-profound hearing loss. Today, even patients with functional residual hearing may receive a cochlear implant.
By using soft-surgery techniques (eg, low drill speeds and slow insertion), the extent of insertional trauma can be reduced. However, long-term changes within the cochlea caused by introducing a foreign body are neither treated nor prevented in current practice.
Although cochlear implant electrode arrays are commonly made from biocompatible polymers, they can elicit an inflammatory response in two ways. First, insertional trauma can induce an acute intracochlear tissue response, resulting in formation of iatrogenic scar tissue around the array. Second, a delayed inflammatory reaction due to the natural host tissue response can lead to encapsulation of the array in a fibrous sheath . In its most pronounced form, the fibrosis can progress to neo-ossification. This new bone formation (NBF) has been observed in animal and histopathologic studies.
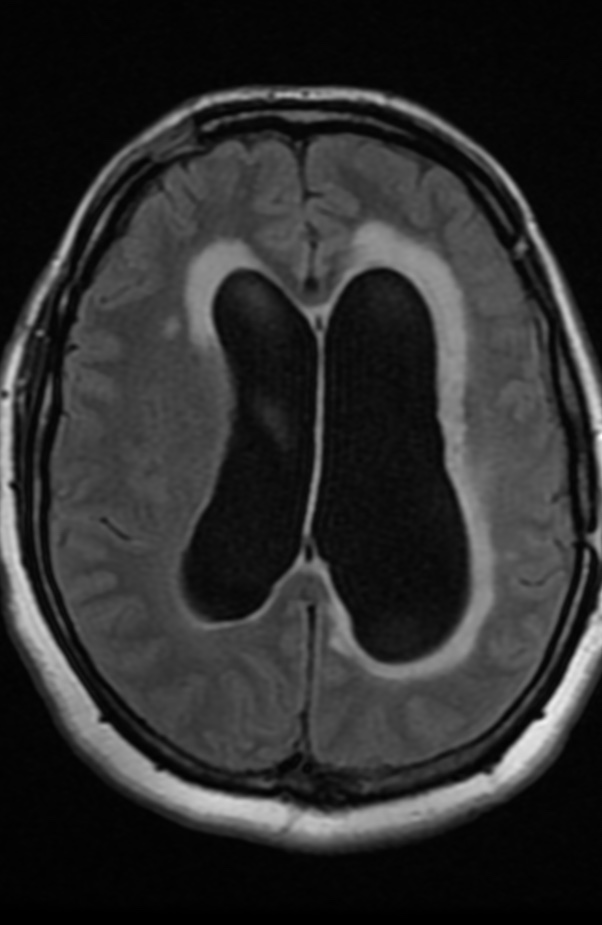
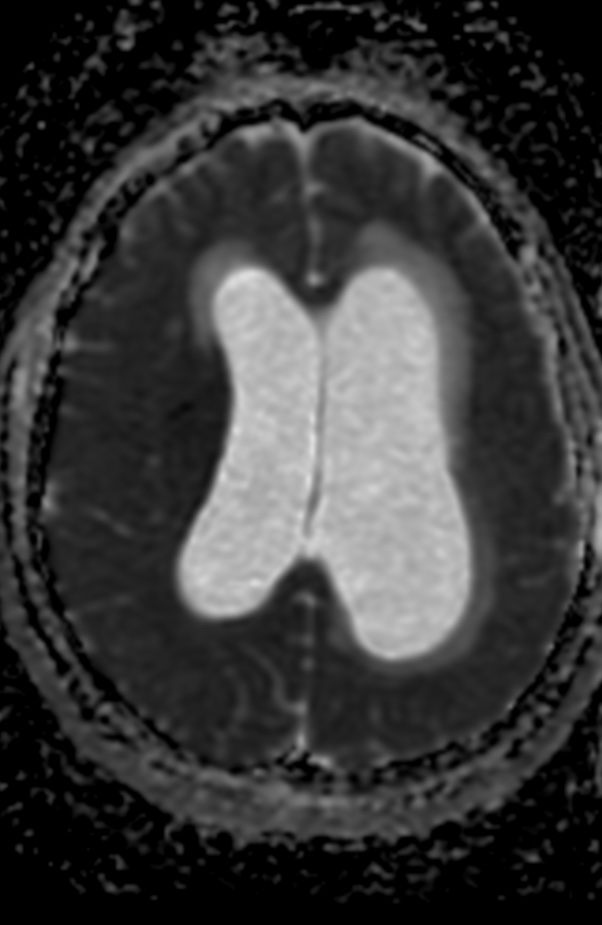
MPD one of the more accurate and powerful method for defining presence of hydrocephalus in-patient even in early stage of occlusion. It has high specificity and sensitivity and capable classify hydrocephalus into grades according to severity.
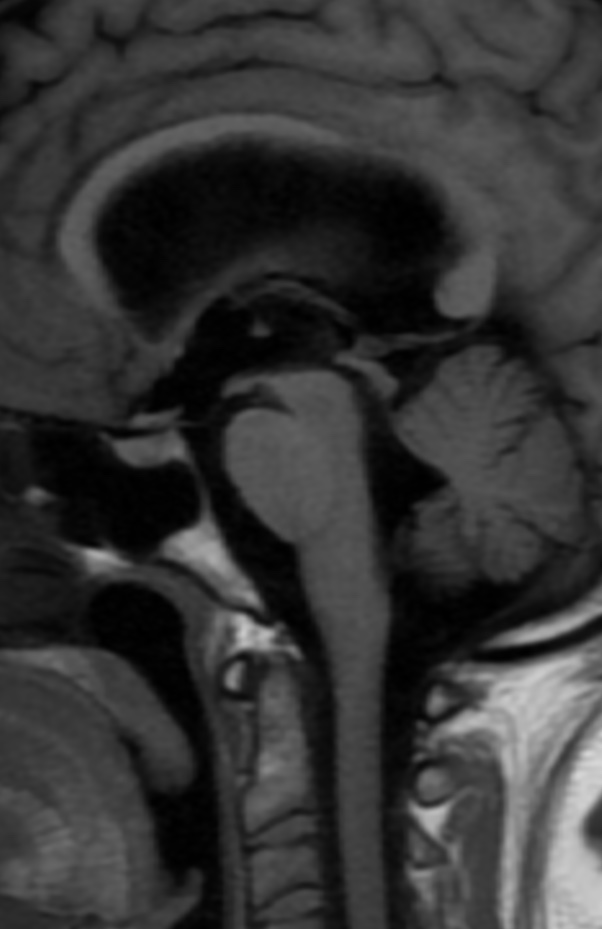
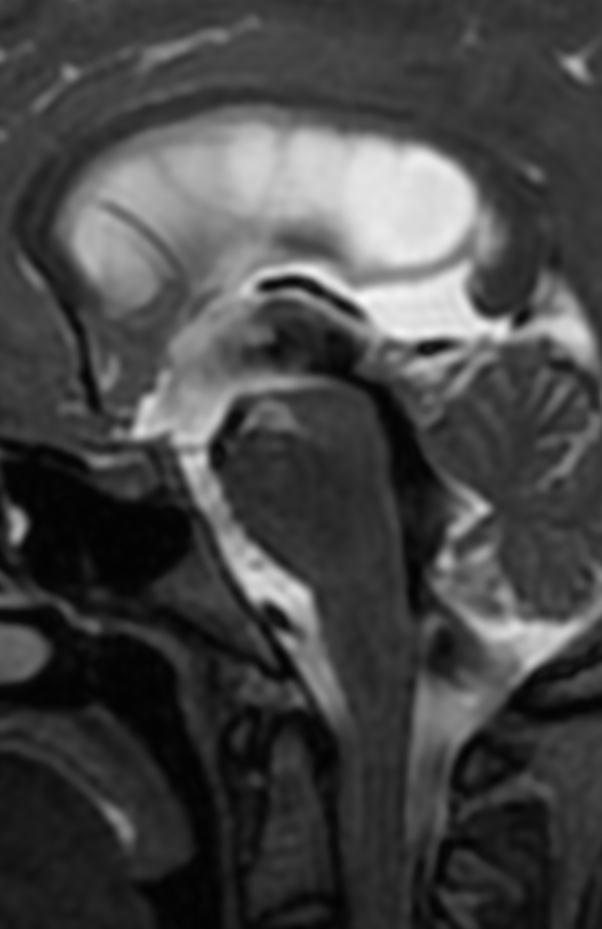
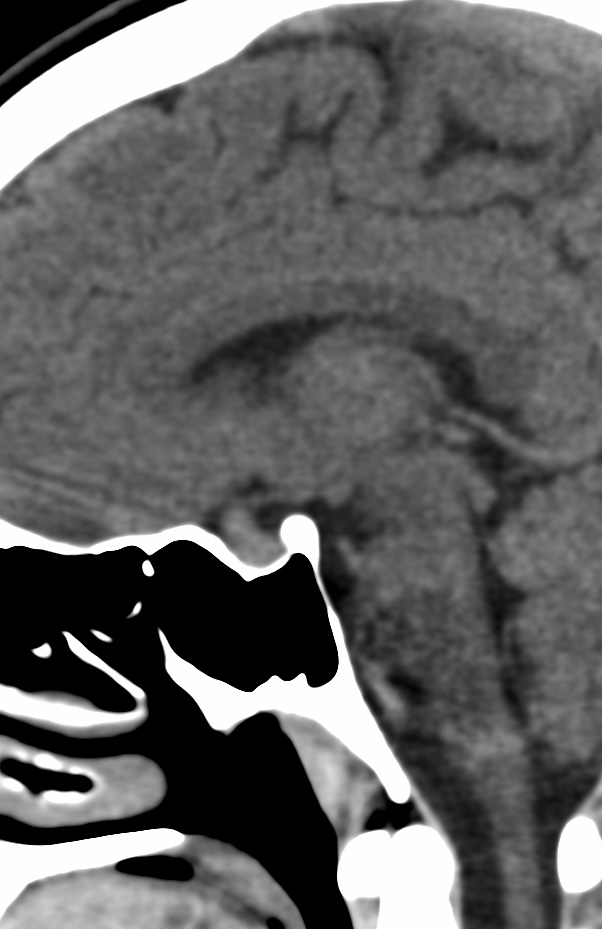
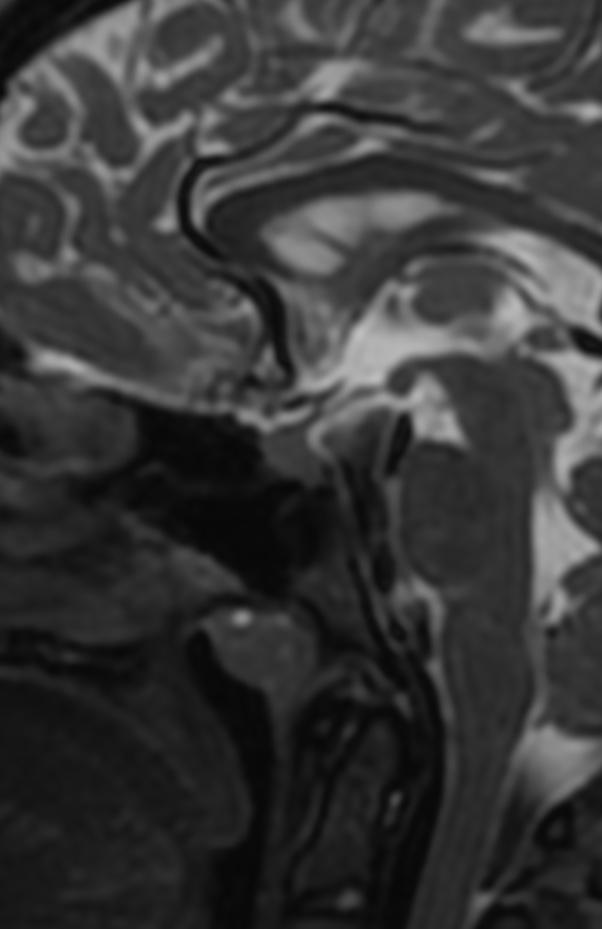
Rathke cleft cyst (RCC) is a benign epithelial cyst believed to originate from the remnants of the Rathke pouch.
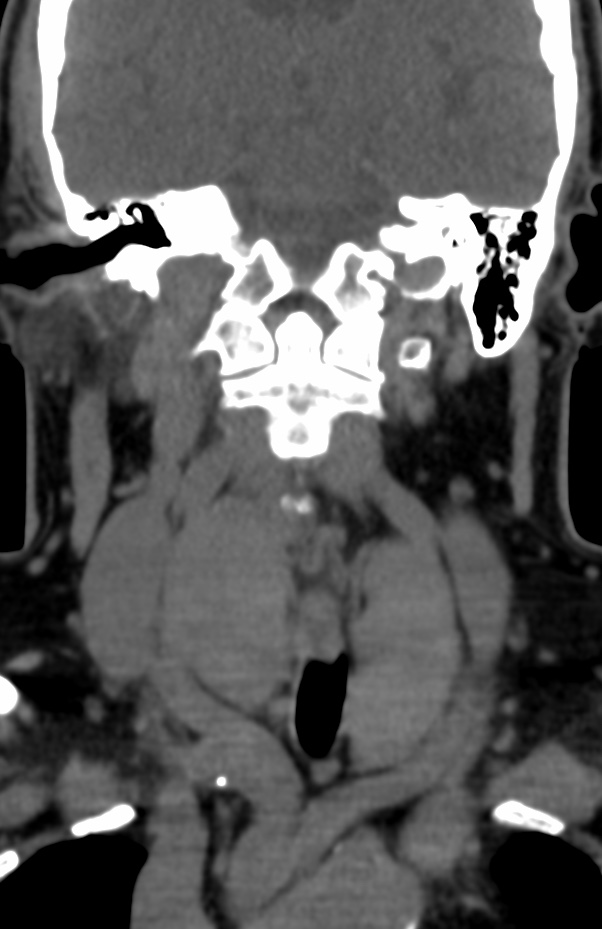
Typical imaging findings include a nonenhancing, noncalcified, intrasellar/suprasellar cyst with an intracystic nodule.
Rathke cleft cysts are most commonly hypodense on CT imaging. the lack of calcification, which helps distinguish RCC from craniopharyngiomas, which are typically calcified (90%). RCC are Hypodense (75%), mixed iso-/hypodense (20%), Hyperdense (5-10%), curvilinear calcification in the wall (10-15%). Does not enhance.






















{kind=link}