Lymphangiomas are rare congenital benign lesions occurring mainly in the head, neck and oral cavity frequently present at birth. Cystic hygromas, however, account for approximately 90% of the lymphangiomas in the head and neck region. Other common sites, outside the head and neck, include the axilla, shoulder, chest wall, mediastinum, abdominal wall, and thigh. They have no predilection for sex or race, and they have no malignant potential. Typical cystic hygromas cause no symptoms unless they enlarge in size or surround or invade adjacent normal anatomic structures. Cystic hygromas may cause symptoms such as feeding problems or breathing difficulties. Cystic hygromas are multilobulated, thin-wall, lymph-containing sacs. The fluid within the sacs is usually clear or amber colored, although occasionally it could be turbid or hemorrhagic.
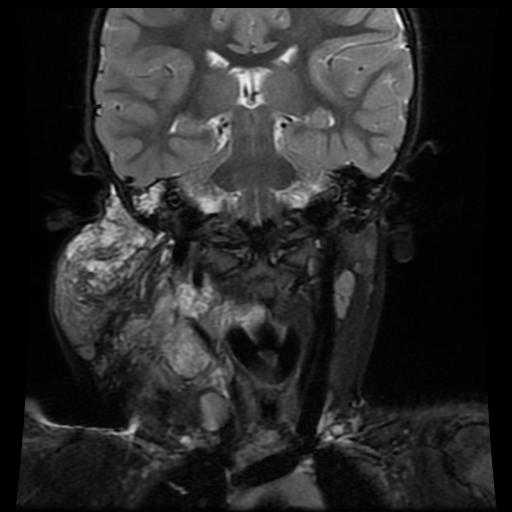
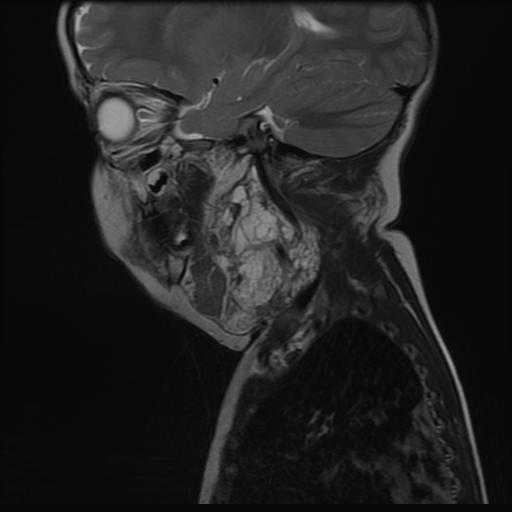
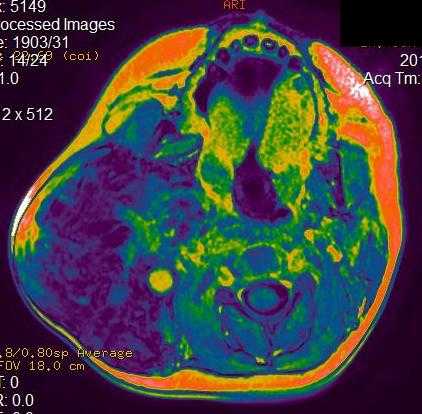
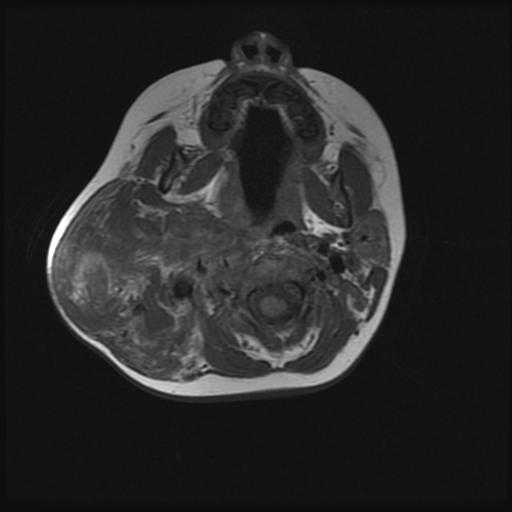
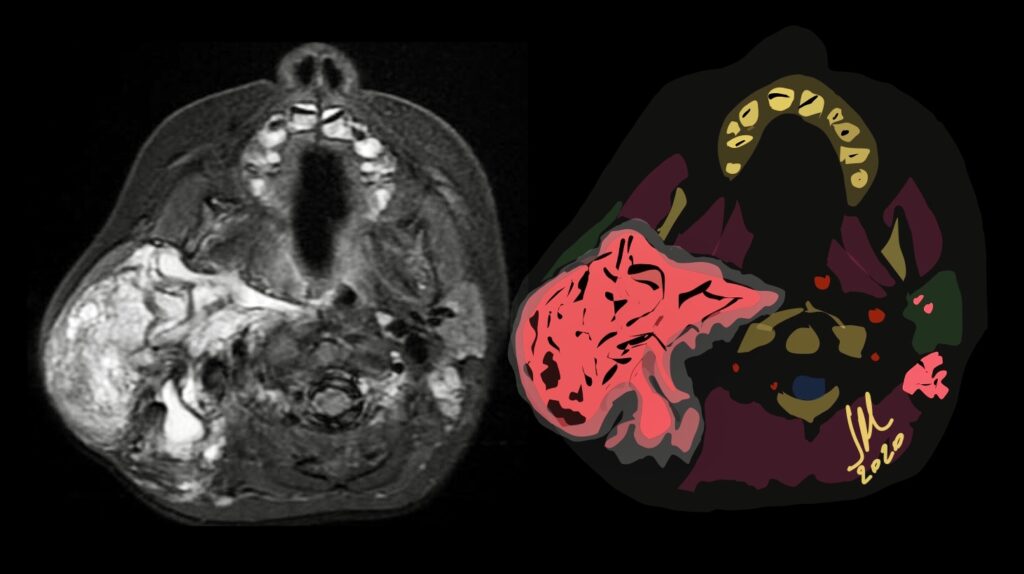
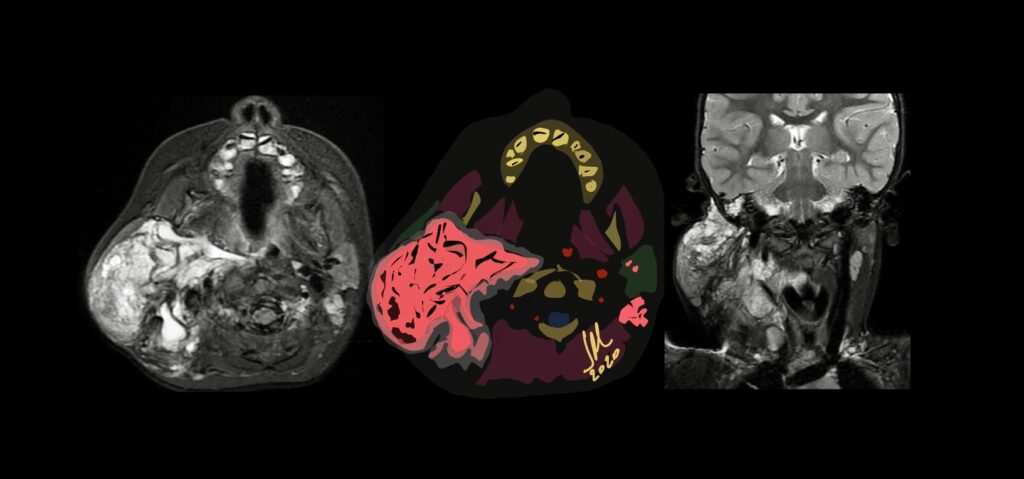
MR imaging is useful to confirm the diagnosis and define the extension of the cystic lesions and their relationship to adjacent structures. A diagnostic dilemma may occur if a cystic hygroma containing a suspicious vascular anomaly is seen in the lower neck or upper mediastinum. In this case, the vascular malformation should be differentiated from a thoracic duct aneurysm.
They consist in localized centres of abnormal development of the lymphatic system. Three theories have been proposed to explain the origin of this abnormality. The first suggests that a blockage or arrest of normal growth of the primitive lymph channels occurs during embryogenesis, the second that the primitive lymphatic sac does not reach the venous system, while the third advances the hypothesis that, during embryogenesis, lymphatic tissue lays in the wrong area